Download
1 / 33
370 likes | 1.32k Vues
Treatment and Prevention of Opportunistic Infections: Options for the Caribbean Region. Excerpted from presentation by Jonathan E. Kaplan, M.D. What is the most frequent serious opportunistic infection in HIV-infected adults in the Caribbean region?. . Toxoplasma gondii encephalitis

E N D
Treatment and Prevention of Opportunistic Infections:Options for the Caribbean Region Excerpted from presentation by Jonathan E. Kaplan, M.D.
What is the most frequent serious opportunistic infection in HIV-infected adults in the Caribbean region? • .Toxoplasma gondii encephalitis • .Tuberculosis • .Pneumocystis jiroveci pneumonia (PCP) • .Cryptosporidium spp. infection • .Hookworm infection
Can you confirm the diagnosis of Pneumocystis jiroveci pneumonia (PCP) in your practice setting? • Yes • No • Don’t know
What clinical specimens are collected to diagnose Pneumocysis infection? • Expectorated sputum • Induced sputum • Bronchial washings • Lung biopsy • Blood cultures
How you confirm cryptococcal infection in your practice setting? • India Ink stain • Culture • Cryptococcal antigen test
Chemoprophylaxis against Pneumocystis jiroveci pneumonia (PCP) with trimethoprim-sulfamethoxazole (TMP-SMZ) can also reduce the incidence of: • Non-typhoidal Salmonella disease • Toxoplasmic encephalitis • Bacterial pneumonia • Isosporiasis • All of the above
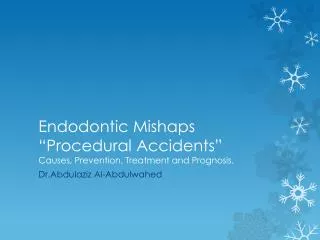
Natural Course of HIV Infection and Common Complications 1000 Asymptomatic 900 Relative level of Plasma HIV-RNA 800 CD4+ T cells 700 TB CD4+ cell Count Acute HIV infection syndrome 600 500 HZV 400 OHL 300 OC 200 PCP 100 TB CMV, MAC 0 0 1 2 3 4 5 1 2 3 4 5 6 7 8 9 10 11 Months Years After HIV Infection
Caribbean Guidelines for the Treatment of Opportunistic Infections in Adults and Adolescents Infected with the Human Immunodeficiency Virus
Oral candidiasis (thrush) Esophageal candidiasis Clotrimazole troches, 10 mg 5 times/day for 7 days Fluconazole, 3-6 mg/kg/day for 1-2 weeks. Chronic maintenance therapy suggested for several months (fluconazole, 200 mg/day) Mucocutaneous Candidiasis: Treatment
Pneumocystis jiroveci (formerly carinii) Pneumonia (PCP) • History: subacute onset (days to weeks) of shortness of breath, dry cough, fever • Physical exam: tachypnea and hypoxemia • CXR typically shows bilateral, diffuse, interstitial pulmonary infiltrates • Diagnosis difficult: requires bronchoscopy or sputum induction and special stains • Treatment: TMP-SMZ (cotrimoxazole, CTX), 15-20 mg/kg/day for 3-4 weeks • For severe cases, add prednisone, 40 mg/day tapering over 3 weeks • Chronic maintenance therapy required (CTX 160/800 mg/day)
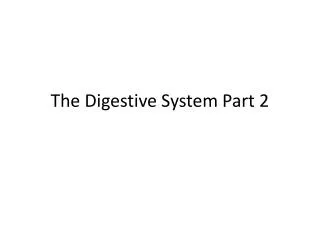
AFB Smear AFB (shown in red) are tubercle bacilli
Tuberculosis in HIV-Infected Persons • Causes 11% of HIV-related deaths worldwide • Can occur at any CD4 count • Clinical presentation increasingly atypical as CD4 count declines • In resource-poor areas, a significant percentage of newly-diagnosed HIV-infected persons will be found to have active TB • Should always consider TB in an HIV-infected persons with a pulmonary infiltrate
Bacterial Pneumonia in HIV-Infected Persons • About 8 times more common in HIV-infected vs non-HIV-infected persons • Pneumococcal bacteremia about 100 times more common • Can occur at any CD4 count • Common etiologies: S. pneumoniae, H. influenzae, P. aeruginosa, S. aureus • Treatment: penicillin/ampicillin +/- aminoglycoside; or cephalosporin
Cryptococcal Meningitis • History: severe headache, fever, mental disturbance • Physical exam: no focal neurological signs • Differential: bacterial, TB • LP: high opening pressure, elevated protein, low glucose, organisms • Treatment: amphotericin x 2 wks, then fluconazole x 8-10 weeks • Chronic maintenance therapy: fluconazole, 200mg/day
Cerebral toxoplasmosis • History: headache, fever, confusion, motor weakness • Physical exam: focal neurological signs • Diagnosis: demonstration of multiple mass lesions on CT or MRI • Treatment: pyrimethamine plus sulfadiazine plus folinic acid for 8 weeks • Chronic maintenance therapy: same
WHO Integrated Management of Adolescent and Adult Illness • Consists of 4 modules: Acute Care, Chronic HIV Care with ARV Treatment, General Principles of Good Chronic Care, Palliative Care • Posted on WHO website in Dec 2003 (available at www.who.int/3by5/publications/imai/en/) • Acute Care: syndromic treatment of illness - appropriate for all patients, but with attention to HIV; - oriented to Health Center level
Tuberculosis (“paradoxical reaction”) Mycobacterium avium complex (MAC) Pneumocystis jiroveci pneumonia (PCP) Toxoplasmosis Hepatitis B Hepatitis C Cytomegalovirus (CMV) Varicella Zoster Virus (VZV) Cryptococcosis Progressive multifocal leukoencephalopathy (PML) Immune Reconstitution Syndromes
Caribbean Guidelines for the Prevention of Opportunistic Infections in Adults and Children Infected with Human Immunodeficiency Virus
What diseases may be prevented? • Pneumocystis jiroveci pneumonia (PCP) • Cerebral toxoplasmosis • Tuberculosis • Mycobacterium avium complex (MAC) disease • Disease caused by S. pneumoniae
Prophylaxis against PCP • Survival benefit demonstrated; first recommended in 1989 • Eligibility criteria: CD4 count <200 cells/uL or <14% or history of oral candidiasis • Drug of choice: TMP-SMZ (CTX) 160/800 (1 double-strength tab) qd
Cotrimoxazole Prophylaxis Can prevent: • Pneumocystis jiroveci pneumonia • Cerebral toxoplasmosis • Disease caused by S. pneumoniae • Disease caused by non-typhoid Salmonella • Nocardiosis • Isosporiasis • Malaria
CTX Prophylaxis: Other Advantages • Cheap ($1 US/month) • Easy to administer: only contraindication is history of sulfa allergy • Main adverse reaction is skin rash, but uncommon in dark-skinned persons • Clinical monitoring is adequate • Adherence is not critical • Experience taking daily medication; good preparation for ART
Isoniazid Preventive Therapy (IPT) • International “best practice” • If skin testing available, may reserve for persons with positive tuberculin skin test (> 5 mm induration) • Otherwise, IPT suggested for all HIV-positive patients living in countries with high prevalence of TB • IPT also suggested for HIV-positive persons exposed to case of active TB • Give isoniazid (INH), 300 mg per day for 9 mo • EXCLUSION OF ACTIVE TB IS CRITICAL
Preventing Disease Recurrence: OIs that Require Preventive Therapy for Life • PCP • Cerebral toxoplasmosis • Systemic (deep) fungal infections: cryptococcosis, histoplasmosis • Disseminated MAC infection • CMV disease
Pathogen Pneumocystis jiroveci Mycobacterium tuberculosis Indication HIV-exposed/infected children 1-12 months; older HIV-infected children with CD4< 15% Contact with person with TB Prophylaxis against First Episode of Opportunistic Disease in HIV-exposed/infected Infants and Children Drug Cotrimoxazole Isoniazid