Alzheimer’s Disease The Cholinesterase Inhibitor Medications
360 likes | 882 Vues
Alzheimer’s Disease The Cholinesterase Inhibitor Medications. Diagnosed Dementia Patients. 2.5. 2.0. 1.5. Diagnosis visits (millions). 1.0. 0.5. 0. 1995. 1996. 1997. 1998. 1999. 11/99 to. 10/2000. PCPs. Neurologists. Psychiatrists. All others.

Alzheimer’s Disease The Cholinesterase Inhibitor Medications
E N D
Presentation Transcript
Alzheimer’s DiseaseThe Cholinesterase Inhibitor Medications
Diagnosed Dementia Patients 2.5 2.0 1.5 Diagnosis visits (millions) 1.0 0.5 0 1995 1996 1997 1998 1999 11/99 to 10/2000 PCPs Neurologists Psychiatrists All others Source: National Disease and Therapuetic Index (Diagnosis codes: 3310, 2900, 2901, 2902, 2903, 2904).
Cholinergic Hypothesis • Role • Acetylcholine (ACh) is an important neurotransmitterin brain regions involved in memory • Impact • Loss of ACh in AD correlates with impairment of memory • Treatment approach • Enhancement of cholinergic function may stabilize or improve cognitive function and may affect behavior and daily functioning Mayeux R et al. N Engl J Med. 1999;341:1670-1679.
Cholinergic Hypothesis • Cholinergic deficiency contributes to cognitive decline in AD • It may contribute to behavioral symptoms of AD • Psychosis-agitation • Apathy-indifference • Disinhibition • Aberrant motor behavior
Cholinergic Hypothesis (cont’d) • Atrophy of the nucleus basalis of Meynert, the source of choline acetyltransferase, causes deficit • Other neurochemical and neurohistologic abnormalities contribute to the psychopathology of AD • Cholinergic therapy may partially improve behavioral symptoms of AD • Cholinergic therapy does not interrupt the disease process
Current Medications Used to Treat AD *Paxil 3% Other25% *Zyprexa 3% *Zoloft 3% Vitamin E 3% *Ativan 4% Aricept44% *Haldol 6% *Risperdal 9% *These uses are investigational. Source: National Disease and Therapeutic Index, 1998.
Cholinesterase Inhibitors • FDA-approved agents: tacrine, donepezil, rivastigmine • Doses • Tacrine: 80 to 160 mg/d • Donepezil: 5 and 10 mg/d • Rivastigmine: 6 to 12 mg/d • Galantamine: 20 to 50 mg/d • Efficacy in mild/moderate AD • Limited information on long-term treatment and in late-stage disease • May be helpful in Lewy body disease Krall WJ, Sramek JJ, Cutler NR. Ann Pharmacother. 1999.
Cholinesterase Inhibitors (cont’d) • Side-effect profiles are similar • Tacrine: liver toxicity, nausea, vomiting, diarrhea • Donepezil: nausea, vomiting, diarrhea, muscle cramps • Rivastigmine: nausea, vomiting, diarrhea, headache, dizziness • Galantamine: nausea, vomiting, agitation, sleep disturbances
Hypothesized Treatment Effectin Alzheimer’s Disease Untreated Cholinesterase Inhibitor (CI) 6 – 4 – 2 – 0 – -2 – -4 – -6 – -8 – -10 – -12 – -14 – -16 – Cognitive Function(ADAS –Cog) 1 year 2 years
Acetylcholinesterase Inhibitor Development 1993 1994 1995 1996 1997 1998 1999 2000 2001 donepezil(Aricept®) tacrine (Cognex®) rivastigmine (Exelon®) galantamine (Reminyl®)
Characteristics ofCholinesterase Inhibitors Dose Drug Binding escalation Dosing tacrine Noncompetitive, 6-week steps qid (Cognex®) reversible donepezil Noncompetitive, 4-6-week step qd(Aricept®) reversible rivastigmine Noncompetitive 2-week steps bid(Exelon®) reversible Davis KL, Powchik P. Lancet. 1995;345:625-630.Aricept® package insert.Exelon® package insert.
Tacrine (Cognex®) • Half-life of 3–5 hours (variable, affected by food intake) • 4-times-daily dosing of 10 to 40 mg (40 to 160 mg/day) • Metabolized by the cytochrome P450 isoenzyme CYP1A2 • Associated with hepatotoxicity (monthly liver testing suggested) Davis KL, Powchik P. Lancet. 1995;345:625-630.Crimson ML. Pharmacotherapy 1998;18(2 pt 2):47S-54S.
Donepezil (Aricept®) • The first second-generation cholinesterase inhibitor • Half-life of 70 hours • Once-a-day dosing of 5 to 10 mg • Metabolized by cytochrome P450 isoenzymes CYP3A and CYP2D6 • Higher doses associated with cholinergic side effects, but generally well tolerated Bryson HM, Benfield P. Drugs Aging. 1997;10:234-239.Aricept® package insert.
Rivastigmine (Exelon®) • Newer second-generation cholinesterase inhibitor • Half-life of 1.5 hours • Dosing (bid) of 3 to 12 mg/day • Metabolism is almost totally independent of the hepatic cytochrome P450 system • Gastrointestinal adverse events are common, including weight loss Exelon® package insert.
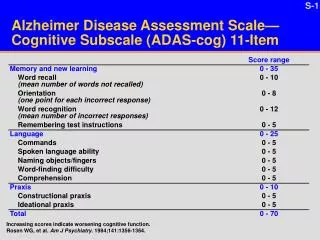
Outcome Scales Used in Phase III Trials of AD Drugs Cognition Alzheimer’s Disease Assessment Scale- Cognitive Subscale (ADAS-cog) Global change Clinician Interview-Based Impression of Change plus Caregiver Input (CIBIC-plus) Activities of daily living Interview for Deterioration in Daily Living Activities in Dementia (IDDD) Progressive Deterioration Scale (PDS) Clinical Dementia Rating-Sum of Boxes (CDR-SB) Behavioral disturbances Neuropsychiatric Inventory (NPI) (ADL)
Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-cog) • Primary outcome measure • A validated, sensitive, and psychometric measure • Contains 11 items that measure cognitive change • Scoring range is 0–70; higher scores = greater cognitive impairment • Efficacy is measured as mean change from baseline Rosen WG et al. Am J Psychiatry. 1984;141:1356-1364.
Clinician Interview-Based Impression of Change plusCaregiver Input (CIBIC-plus) • Evaluates 4 areas: cognition, behavior, daily functioning, general psychiatric symptoms • Scores range from 1 (markedly improved) to 7 (markedly worse) Schneider LS et al. Alzheimer Dis Assoc Disord. 1997;11(suppl 2):S22-32.
Tacrine Safety • Adverse gastrointestinal effects (somewhat alleviated by concomitant food intake) • Elevated liver transaminase levels (ALT) • 25%–30% of patients with ALT > 3 times the upper limit of normal • Monitoring of liver function required Farlow M et al. JAMA. 1992;268:2523-2529.Knapp MJ et al. JAMA. 1994;271:985-991.
Placebo 7.8% 26.8% 57.7% Donepezil 5 mg/day 15.4% 37.8% 78.7% Donepezil 10 mg/day 25.2% 53.5% 81.1% Donepezil: Percentage of Patients With Improvement in ADAS-cog (Rogers) Change in ADAS-cog (LOCF*) 4 7 0† Treatment group Rogers SL et al.Neurology. 1998;50:136-145. * Last observation carried forward.† Includes patients who did not improve or decline.
Donepezil Safety • Individual adverse events that occurred significantly more frequently with donepezil 10 mg than with placebo: • Nausea (17%) • Diarrhea (17%) • Vomiting (10%) • Fatigue (8%) • Muscle cramps (8%) Rogers SL et al. Neurology. 1998;50:136-145.
Donepezil Safety (cont) • In the largest trial (N = 818), digestive system and nervous system adverse events occurred more frequently with donepezil 5 mg and 10 mg than with placebo • Digestive system = 36% vs 24% • Nervous system = 38% vs 29% Burns A et al. Dement Geriatr Cogn Disord. 1999;10:237-244.
Donepezil Summary • Donepezil (5* and 10 mg) improves cognition and global function in patients with mild-to-moderate AD • Long-term efficacy is maintained for up to 50 weeks • ADL may be partially maintained by donepezil • Donepezil is generally safe and well tolerated * In the largest trial, donepezil 5 mg was significantly betterthan placebo using the ADAS-cog scale, but scoresworsened from baseline.
Rivastigmine Safety • During the maintenance phase, adverse events with rivastigmine 6–12 mg (1–4 mg)* compared with placebo were: • Dizziness, 14% (8%) vs 4% • Nausea, 20% (8%) vs 3% • Vomiting, 16% (5%) vs 2% • Dyspepsia, 5% (6%) vs 1% • Sinusitis, 4% (1%) vs 1% * p < 0.05 vs placebo for all events except rivastigmine 1–4 mg for dizziness and sinusitis (not different from placebo). Corey-Bloom J et al. Int J GeriatrPsychopharmacol. 1998;1:55-65.
Rivastigmine Safety (cont) • Rivastigmine was generally safe andwell tolerated • There was no evidence of hepatotoxicity • Fewer adverse events were observed with concomitant food administration versus administration without food • In addition to nausea and vomiting, rivastigmine was associated with significant weight loss Exelon [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2000.
Rivastigmine Summary • Rivastigmine (6–12 mg) improves cognitionand global function in patients withmild-to-moderate AD • Positive effects on ADL have been observed in some studies • Rivastigmine is generally safe and well tolerated, although cholinergic side effects occur at high doses
Galantamine (Reminyl®) • Galantamine has a dual mechanism of action • Competitive inhibition of acetylcholinesterase1 • Allosteric modulation of presynaptic and postsynaptic nicotinic receptors2 • Galantamine improves major aspects of AD (eg, cognition, behavior, function)1 • Galantamine is generally safe and well tolerated1 1. Tariot PN et al. Neurology. 2000;54:2269-2276. 2. Maelicke A, Albuquerque EX. Eur J Pharmacol. 2000;393:165-170.
Dual Mechanism of Action N = nicotinic M = muscarinic ACh = acetylcholine Presynaptic nerve terminal M receptor N receptor Galantamine Galantamine ACh and other neurotransmitters • Choline • Acetic acid ACh Postsynaptic nerve terminal N receptor M receptor Maelicke A, Albuquerque EX. Eur J Pharmacol. 2000;393:165-170. Tariot PN et al. Neurology. 2000;54:2269-2276.
Galantamine: Potential Advantages of Nicotinic Receptor Modulation • May increase release of ACh • Release of other neurotransmitters also increases • May have a neuroprotective effect Maelicke A, Albuquerque EX. Eur J Pharmacol. 2000;393:165-170.
Galantamine Safety (cont) Galantamine Galantamine Placebo 16 mg/day 24 mg/day (n = 286) (n = 279) (n = 273) Adverse events* (%) (%) (%) Nausea 4.5 13.3 16.5 Vomiting 1.4 6.1 9.9 Anorexia 3.1 6.5 8.8 Agitation 9.4 10.0 8.1 Diarrhea 5.9 12.2 5.5 Tariot PN et al. Neurology. 2000;54:2269-2276. * 5% of patients receiving galantamine and more often than in patients receiving placebo.
GI Adverse Events • Nausea: incidence related to treatment initiation and dose escalation • Typically transient, resolving within 1 week • Rarely severe • Weight loss: reported as an adverse event in 5% of patients, with none discontinuing treatment Reminyl® package insert.
Comedication • Minimal potential for clinically relevant drug interactions • No effect on kinetics of digoxin or warfarin • As with other cholinergics, galantamine should be used with caution in patients with heart block or sick sinus syndrome
Agents in Development • Memantine–NMDA receptor antagonist • Improvement in patients with severe AD and VaD1 • Recent phase III trials indicate significant improvement compared with placebo in CIBIC-plus scores2 • Patients with moderately severe and severe AD benefited the most 1. Winblad B, Portis N. Int J Geriat Psychiatry. 1999;14:135-146. 2. Reisberg B. World Alzheimer Congress, 2000.
Agents in Development (cont) • Immunization against b-amyloid1 • Huprine X—acetylcholinesterase inhibitor2 • Xanomeline patch—m1/m4 muscarinic receptor agonist3 • AIT-082 (purine hypoxanthine derivative)—increases neurotransmission4 • COX 2 inhibitors—neuroinflammation therapy5 • Protease inhibitors—target g-secretases to prevent amyloid formation6 1. Schenk DB et al. Nature. 1999;400:173-177. 2. Camps P et al. Mol Pharmacol. 2000;57:409-417. 3. Shannon HE et al. Schizophr Res. 2000;42:249-259. 4. Lahiri DK et al. Ann NY Acad Sci. 2000;903:387-393. 5. O’Banion K. World Alzheimer Congress, 2000. 6. Dovey HF et al. J Neurochem. 2001;76:173-181.
Current Treatment Summary • Cholinergic agents initially improve and transiently maintain cognitive abilities in patients with mild-to-moderate AD • Cognitive abilities worsen over time, indicating treatment does not stop (but may delay) the progression of AD • New treatments that maintain cognitive ability and stop the progression of AD are needed
Referrals SHANDS at UF Geriatric Psychiatry Inpatient Unit Intake and Referral Line 352-265-5411 UF Psychiatry Clinical Trials Program 1-877-STUDY94