Download
1 / 25
0 likes | 13 Vues
If you need to know more about Polycystic Ovary Syndrome Diagnosis? Contact- Jindal IVF Chandigarh. Book an appointment call us: 91 9418127128

E N D
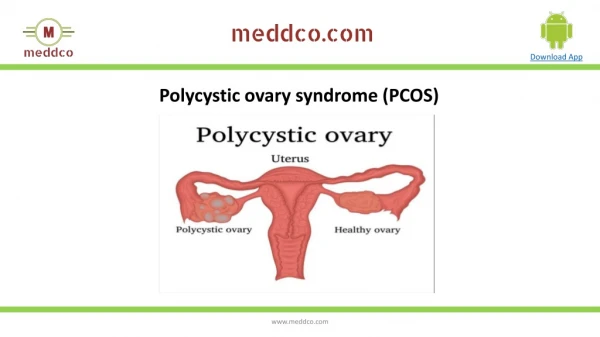
Polycystic Ovary Syndrome Diagnosis Shimla, FOGSI 25.06.11 Umesh N. Jindal Jindal IVF & Sant Memorial Nursing Home Chandigarh
History • Described first in 1935 • Histology : • Twice cross-sectional area • Same number of primordial follicles • Double the developing and atretic h follicles. • 50 % thick tunica • 4 fold greater number of hilar call nests
SpectrumofclinicalconditionsassociatedwithPCOS Infertility PCOS DUB Anovulation Obesity Hypertension Diabetes MS Acne Cancers Hirsutism InsulinResistance Atherosclerosis Alopecia CVD Sleep Apnea Depression Fatty liver
Functional disorder • Any chronic anovulatory state will lead to a polycystic picture provided HPO axis is intact. • Hyper estrogenism and / or hyper androgensim due to any cause will lead to PCO.
Hormone Status • Estradiol fluctuate but remain within normal range. • Increased Estrone peripheral conversions. • Increased Testosterone • Increased Androsternedione Ovary LH dependent • Increased17-OHP • Increased DHEA • Increased DHEA-S Adrenal
Causes of PCOS Genetic Gn regulation and action Weight and energy regulation PCOS Complex metabolic disorder Insluin secretion and action Androgen synthesis and regulation Environmental
Pathophysiology • Complex metabolic disorder • Functional derangement of follicular development • Increased estogens and androgens, LH and loss of cyclicity due self propogating feed back loop. • Insulin resistance in 70 %. • Polygenic inheritance.
Evaluating Androgen excess Clinical Hyperandrogenemia • Hirsuitism • 60-70% • More gradual • Variation with age and ethnicity • Ferrimen and Gallway score->15 severe
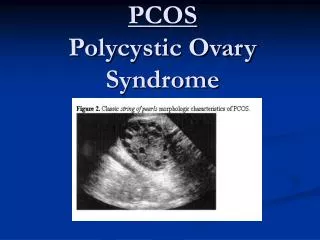
Polycystic Ovarian Morphology • Early follicular phase(day3-5) • Oligo/Amenorrhoeic-At random or3-5 days • Stromal area/total area ratio and or increased stromalechogenesity • The usefullness of 3-D,Doppler or MRI (Ultrasound assessment of the polycystic ovary-International consensus definition-Human reproduction;9:505-13)
Evaluating PCOM Swanson and Co-Workers-1981 • General population-20-33% • > 12 follicles at 2 - 9 mm in at least 1 ovary • Volume > 10cc • If a follicle is >10mm, repeat scan next cycle. • Transvaginal is preferable • Does not apply to women on OC pills • Single ovary-sufficient to diagnose
PCOM PCOM (Polycystic Ovarian Morphology)
Clinical features • Obesity-BMI>25 in 35-50% • Android appearance • Waist to hip ratio • Acanthosis Nigricans-Non specific • HAIR-AN SYNDROME • Hyperpigmented velvety patch-nape of the neck,axilla,inner thigh and vulva
Biochemical Investigations Gonadotrophins-LH/FSH • Increase in amplitude and frequency of LH • Elevated in 95% • LH increased in 60-70% • ?Reliability of a single measurement • Increased LH levels and its treatment-controversial • Lack on agreement on abnormal result
Biochemical investigations • 2 hr GTT-F-110-125mgm/dl 2hr-140-199mgm/dl With severe stigmata of insulin resistance and hyperandrogenemia or undergoing ovulation induction • Fasting insulin->25microIU/ml • Fasting G/I ratio of 4.5 or less (Suggested evaluation in PCOS-ACOG2009)
Biochemical investigations Tests for metabolic syndrome(Updated adult t/t panel lII) • Cholestrol,LDL • HDL<50mgm/dl • Triglycerides>150mgm/dl • BP-130/85 • F blood glucose>100mgm/dl • Waist circumference>35 inches (Suggested evaluation in PCOS-ACOG2009)
Diagnosis of exclusion • Hypergonadotrophichypogonadism • Hypogonadotropichypogonadism • Non classic congenital adrenal hyperplasia • Suspected PCOS-1-19% • Screening-17OHP-<200ng/dl,>500 certain • ACTH stimulation test-25USP • 17OHP>1000 • CUSHING SYNDROME 24 hour free cortisol and 17 hydroxysteroids
Diagnosis of exclusion • Adrenal and ovarian tumours • Rapid virilization • Testosterone >200ngm/dl • DHEAS >700ng/dl • Imaging techniques • ? Hyper prolactinamia • ?Hypothyroidism
Complete Evaluation • HISTORY-Menstral disturbances, Hyperandrogenism, Infertility, weight gain, Galactorrhoea, Symptoms of hypothyroidism, Drug intake, Family history • Examination-BMI, Type of obesity, Hypertension, Hirsuitism, Signs of virilization, Signs of Cushings disease, Galactorrhoea, Acanthosis nigricans, Abdominal examination, PV /PR Examination
Complete Evaluation • Free testosterone • Total testosterone • DHEAS • LH/FSH Ratio • 17OH progesterone • Test for hyperinsulinemia • Test for dyslipidemias • Prolactin • TSH
Conclusions • Early diagnosis and intervention is imperative • Rotterdam criteria should be used • Somatic or Lab Hyperandrogenism • Oligo-anovulation • Polycystic Ovarian Morphology • Exclude • Non-classical 17-hydroxylase deficiency, adrenal tumor, Cushing’s, prolactinemia, thyroid disorders, hypothalamic amenorrhea Make a diagnosis of PCOS before starting treatment