Download
1 / 15
150 likes | 165 Vues
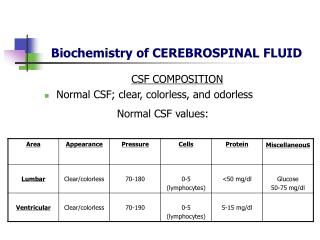
This study aims to describe the cerebrospinal fluid (CSF) findings in infants ≤12 months old with confirmed pertussis. The CSF parameters, including cell count, protein, glucose, and culture results, were analyzed. No cases of bacterial meningitis or intracranial hemorrhage were found. Elevated CSF protein was a common finding in infants with pertussis.

E N D
Cerebrospinal Fluid Findings in Infants with Pertussis Tina T. Chu, MD, Jesse Groh, MD, Andrea T. Cruz, MD, MPH Department of Pediatrics Baylor College of Medicine Houston, Texas
Abstract Infants with pertussis often receive extensive medical and laboratory evaluation for fever or apnea caused by this infection. Cerebrospinal fluid (CSF) findings in infants have not been reported. The objective of this 5-year retrospective review is to describe the CSF findings in infants < 12 months of age with polymerase chain reaction (PCR) confirmed pertussis in whom CSF was obtained. 39 (19.6%) of the 199 infants with positive pertussis PCR received a lumbar puncture (LP). Reasons for performing LP included apnea (62%), toxic appearance (38%), fever and age < 1 month (26%), and altered mentation (10%). 24 (62%) children had elevated CSF protein. No child had bacterial meningitis hypoglycorrhachia, bacteremia, or intracranial hemorrhage. Length of stay and duration of parenteral antibiotics were not significantly different in children with normal versus abnormal CSF parameters. In conclusion, elevated age normalized CSF protein was a common finding in infants with pertussis.
Background • The greatest burden of pertussis disease occurs in infants • Over 2600 admissions annually • 86% of hospitalizations: infants ≤ 3 months • 95% of cases: requiring mechanical ventilation • Pertussis symptoms are often atypical or nonspecific (cyanosis, apnea) and prompt examination of the cerebrospinal fluid (CSF) • CSF profiles in infants with pertussis have not been previously described
Objective To report the cerebrospinal fluid findings of infants with pertussis and parapertussis
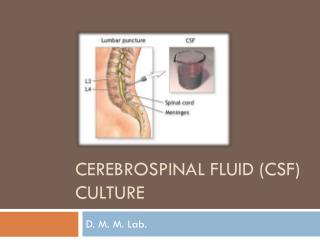
Methods • Retrospective review of children 0-12 months of age seen at Texas Children’s Hospital (TCH) from January 1, 2005 to December 31, 2008 with PCR confirmed Bordetella pertussis infection in whom CSF was obtained • Molecular pathology database accessed to identify those patients in whom CSF was obtained and sent for routine studies (cell count/differential, protein, glucose, Gram stain, and culture) • Data abstracted from medical records: • Demographics • Symptoms • Laboratory and radiographic evaluation • Clinical course
Materials and Methods • Abnormal CSF parameters were determined by patient age • CSF pleocytosis defined as white blood count (WBC): • ≥ 25 cells/μL in neonates ≤ 28 days • ≥ 10 cells/μL in infants > 28 days • Elevated CSF protein defined as: • > 108 g/dL if < 8 days • > 90 g/dL if 8-30 days • > 77 g/dL if 31-60 days • > 60 g/dL if 61-90 days • > 40 g/dL if 91-180 days • Statistical analyses performed using STATA 10 (Stata, Inc., College Station, TX). Frequencies calculated for categorical variables. Means/medians calculated for continuous variables. Student t-test used to compare continuous variables. Differences in proportions between groups calculated using chi-square or Fisher’s exact test and reported with 95% confidence intervals
Patient Demographics • 39 with pertussis or parapertussis received LP • Mean patient age: 43 days (range 16-113 days) • Patient demographics: • 51% female • 67% Hispanic • 20% non-Hispanic black • 13% non-Hispanic white • No children had underlying medical problems • Pertussis immunizations: • 4 not up-to-date • 33 (85%) had not had any due to age < 60 days • 72% with ill contacts with pertussis-like illnesses
Results • Most common symptoms: • cyanosis (62%) • apnea (46%) • fever (31%; median 101.3°F) • rhinorrhea (31%) • Mean symptom duration: 9.4 days (range: 2-28 days) • Indications for LP: • apnea (62%) • toxic appearance (38%) • fever and age < 29 days (26%) • prior to receipt of antibiotics for other infections (26%) • 3 with presumed urinary tract infections (UTIs) • 7 with pneumonias (5 lobar, 2 interstitial)
Breakdown of PCR-Confirmed Pertussis Patients 239 Children with Confirmed Pertussis or Parapertussis, 2004-2008 211 < 1 year 28 ≥ 1 year 172 no CSF 39 CSF obtained† † 15 CSF normal 24 CSF abnormal* 4 ↑WBC 24 ↑ protein 0 ↓glucose † : 36 children had B. pertussis, 2 had B. parapertussis, and 1 child had both B. pertussis and B. parapertussis *: four patients had > 1 abnormal cerebrospinal fluid (CSF) parameter
Results • All pertussis infants with CSF obtained were admitted • Abnormal CSF findings: 24/39 (62%) — all with elevated protein • No hypoglycorrhachia, positive CSF gram stain/bacterial culture, or bacteremia • 2 traumatic LPs (> 500 cells/mm3) • 4 had CSF pleocytosis • 1 with PCR-positive enterovirus of the CSF • 1 nasal wash confirmed enterovirus • 2 no etiology identified • 7 had pneumonia (2 rhinovirus, 1 picornavirus) • 1 had a UTI • No significant differences between CSF cell counts, glucose, or culture results or in microbiologically or virologically confirmed infections in children with normal vs. abnormal CSF protein
Discussion • Our finding of increased CSF protein is difficult to explain and was unlikely due to: • Concomitant pyogenic bacterial infections (No meningitis or bacteremia) • Only 1 UTI and 5 lobar pneumonias. • A minority of children with elevated CSF protein had concomitant viral infections • Hypoxic CNS injury from apnea or paroxysms: no evidence on those with CNS imaging • Hyperthermia: no documented temperatures >104°F • Seizures: no witnessed seizures • Traumatic LPs: only 2 of 24 children had CSF RBC/mm3 > 500 • Evaluation and clinical management of a toxic-appearing infant should not be limited by a positive pertussis or parapertussis PCR, but it is useful for to be cognizant that abnormal CSF protein can be seen in association with these infections
Conclusions • The most common CSF abnormality in infants with pertussis who received a lumbar puncture was elevated CSF protein • While this finding was associated with apnea documented during hospitalization, abnormal CSF findings in this population were not associated with concomitant co-infections or prognosis
References • Namachivayam P, Shimizu K, Butt W. Pertussis: severe clinical presentation in pediatric intensive care and its relation to outcome. Pediatr. Crit. Care Med. 2007;8:207-211. • Surridge J, Segedin ER, Grant CC. Pertussis requiring intensive care. Arch. Dis. Child. 2007;92:970-975. • Lurie G, Reed P, Grant C. When to discharge children hospitalized with pertussis? Acad. Pediatr. 2009; 118-122. • Davis JP. Clinical and economic effects of pertussis outbreaks. Pediatr. Infect. Dis. J. 2005;24:S109-S116. • Cortese MM, Baughman AL, Zhang R, et al. Pertussis hospitalizations among infants in the United States, 1993-2004. Pediatrics. 2008;1221:484-492. • Meehan WP and Bachur RG. Predictors of cerebrospinal fluid pleocytosis in febrile infants aged 0 to 90 days. Pediatr. Emerg. Care. 2008;24:287-293. • Biou D, Benoist JF, Nguyen-Thi C, et al. Cerebrospinal fluid protein concentrations in children: age-related values in patients without disorders of the central nervous system. Clin. Chem. 2000;46:399-403. • Ahmed A, Hickey SM, Ehrett S, et al. Cerebrospinal fluid values in the term neonate. Pediatr. Infect. Dis. J. 1996;15:298-303. • Syrogiannopoulos GA, Grivea IN, Anastassiou ED, et al. Cerebrospinal fluid pleocytosis in young infants with urinary tract infection. Pediatr. Infect. Dis. J. 2001;20:927-930. • Shah SS, Zorc JJ, Levine DA, et al. Sterile cerebrospinal fluid pleocytosis in young infants with urinary tract infections. J. Pediatr. 2008;153:290-292. • Reiber H, Peter JB. Cerebrospinal fluid analysis: disease-related data patterns and evaluation programs. J. Neurolog. Sci. 2001;184:101-122.
Credits • Andrea T. Cruz—Faculty of Infectious Diseases and Pediatric Emergency Medicine, Baylor, Houston, Texas • Mark Ward—Director of Baylor Pediatric Residency Program, Baylor, Houston, Texas

![CEREBRAL CIRCULATION AND CEREBROSPINAL FLUID [CSF]](https://cdn2.slideserve.com/4005143/slide1-dt.jpg)