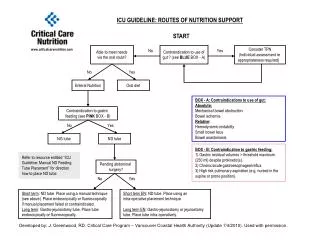
nutrition support
Selecting a method. If the gut works, use itWhen a person is unable to ingest enough food to meet their nutritional needsnutrition support is neededcould be enteral if the gut workscould be parenteral if the gut doesn't work . Enteral Nutrition. By way of the GI tractCould beOral Supplements Tube FeedingsNasogastricNasoduodenal or nasojejunalEnterostomiesGastrostomiesPercutaneous Endoscopic Gast.(PEG)JejunostomiesMultiple Lumen tubes.


nutrition support
E N D
Presentation Transcript
1. Nutrition Support
3. Enteral Nutrition By way of the GI tract
Could be
Oral Supplements
Tube Feedings
Nasogastric
Nasoduodenal or nasojejunal
Enterostomies
Gastrostomies Percutaneous Endoscopic Gast.(PEG)
Jejunostomies Multiple Lumen tubes
4. Selecting an Oral Supplement 1. Degree of inability to meet needs
2. Presence or absence of dysphagia
3. Taste preference or sensitivity
4. Availability of labor and resources for preparation
5. Tolerance to lactose or other components
6. Tolerance of osmotic load
5. Supplement Components Kcals: 250 kcal/ 240 ml portion is the norm
Fat:
Usually Long Chain Triglycerides
Could be MCT if pt doesn�t tolerate fats
Protein:
8 to 14 grams of intact protein
CHO
Form varies: Simple adds sweetness and osmotic load
6. Tube Feedings: Route of Access Several Factors:
1. Length of time required
Short term: usually through nasopharynx
Longer term through enterostomal routes
2. Risk of aspiration
3. Degree of digestion available
4. If there is a planned surgical intervention
7. Nasogastric Route Nasogastric Tube: simplest access
Pt requires functional GI tract and normal gag reflex
French = .33 mm
Can be large bore tube (French #12+)
Used for food, medications and gastric suctioning or
Small bore, pliable tube (5 French)
Greater comfort, but more easily clogged
8. Nasoduodenal or Nasojejunal Tube threads through stomach to duodenum or jejunum
Migration from stomach to duodenum via peristaltic waves may take a few hours to days
Radiologic verification is required
Small bowel feedings require careful selection of enteral formula
9. Enterostomies Surgical Gastrostomy
Catheter is placed through the abdominal wall into the stomach
A balloon is inflated to hold the catheter in place in stomach
Requires good gastric functioning
Can be associated with skin erosion, leakage of gastric contents leading to peritonitis
10. Surgical Jejunostomy Needle jejunostomy(temporary)
Catheter jejunostomy(more permanent)
both reduce risk of pulmonary aspiration
small lumen size of tube difficult to maintain so not often performed
11. Fluid requirements 1ml of water per kcal
35 ml/kg usual body weight
Formulas contain 80 to 85% water
may need to add water as an additional flush
12. Osmolality Intact formulas fall between 300 to 500 mOsmol/kg , approx the same as body fluids
No real concerns with fluid shifts
Hydrolyzed formulas are often higher
up to 900 mOsmol/kg
contributes to extra fluid and electrolyte loss
diarrhea
Proper administration is key
13. Administration of Enterals Continuous drip
Intermittent drip
Bolus feeding
14. Continuous Drip Estimated total kcal needs are made
Rate per hour determined based on the kcal content of formula
2000 kcals needed per day
Formula has 1kcal/cc
2000kcal/1kcal/cc= 2000 cc�s needed
2000cc/24 hrs=83cc�s/hr is set as the goal volume
15. Administration of Continuous Drip Caution when initiating tube feeding
If the gut has not been used lately
If the formula is hyperosmolar
Feedings are typically started at 30 to 50 cc�s/hr
Then advanced 25 to 30 cc�s/hr every 8 to 12 hours until the target rate is obtained
Feedings of 300 to 500 mOsmol/kg can be started at full strength; hyper start slowly
16. Admin of Tube Feeding If intolerance: decrease to previous increment and advance as tolerated
Don�t hang a bag for days
Food born illness
Don�t add new formula on top of old formula
Bag should be changed daily
17. Administration of Tube Feedings If fed into stomach, stomach contents checked every 4 to 8 hours
if residual volume exceeds 100 ml, stomach isn�t emptying quickly and volume admin should be reduced
Risk of pulmonary aspiration
18. Intermittent or Bolus Feedings Quality of Life: A more normal lifestyle with intermittent feedings
Frees pt to be mobile
Figuring intermittent or bolus feedings similar to continuous
Total Kcals determined
Divided by number of hours feeding
General: 4 to 6 feedings @ 20 to 60 min
19. Administration of Bolus or Intermittent Feeding Residuals checked more frequently: every 2 to 4 hours
Few pts can tolerate more than 450 ml per feeding
Pt needs to be monitored for several potential problems
20. Monitoring Tube Fed Pt Weight 3 x wk
Signs of Edema daily
Signs of dehydration daily
Fluid In/Out daily
Cal, Pro, fat, CHO, vit & min 2+/wk
N balance (24-hour UUN) weekly
Gastric residuals (2 to 4 hrs)
21. Monitoring Tube Fed pt Stool output and consistency (daily)
Urine Glucose (every 6 hours until rate is established then daily for Db pt)
Serum electrolytes, BUN, creatinine, blood count (2-3 x wk)
Blood chemistry: total protein, albumin, pre-albumin, Ca, Mg, P, Liver Fxn weekly
22. Tube Feeding Problem Pulmonary Pt with 1800 kcal need
No renal problems or fluid restrictions
gastrostomy in place
Tube feeder with Pulmocare
Pro: casein; CHO: cornstarch and sucrose; Fat: mixed triglycerides
1.5 kcal/ml; 55.2 % kcal from Fat; 28.1 % kcal from CHO;62.5 g Pro/1000cc�s; 78.5% water
? How much Pulmocare?; how much fluid;Pro?
23. Use Nutrition Care Manual http://nutritioncaremanual.org
24. Pulmocare Problem Osmolality is 475 mOsmol/kg
How would you administer this?
What would you monitor to determine tolerance?
What would you monitor to determine if needs were met?
25. Parenteral Nutrition If pt is unable to receive nutrients via the GI tract
Then Parenteral Nutrition is Appropriate
26. Parenteral Access Peripheral Access:
Arm (or leg)
900 mOsm/kg upper limit of acceptable
Higher concentrations cause vein to become inflamed and collapse.
PICC(Peripherally Inserted Central Catheter)
Higher concentration is possible
End of lumen is threaded to a larger vessel with greater dilution capacity
27. Parenteral Access Short Term Central Catheter
Subclavian vein central catheter
line inserted into Subclavian and threaded to the superior vena cava
Provides maximum dilution of parenteral solution and no damage to the vein lumen
Risk of infection
28. Parenteral Access Long-term Access
When access is required for many months or longer, a permanent catheter is surgically placed
A port is imbedded under the skin which is accessible
29. Terminology with Parenteral Solutions D Dextrose
W Water
NS Normal Saline (0.9%) NaCl solution 0.9 g NaCl/ 100 ml
D5W 5% Dextrose solution in water
(5 g Dextrose in 100 ml water)
D51/2 NS 5% Dextrose in 1/2 Normal Saline (0.45 g NaCl in 100 ml Water)
30. Nutrients in Parenteral Soln Protein
Combination of essential and non-essential aa�s
Generally 15 to 20 % of total Kcal needs in most solutions
Often a 10% amino acid solution is used
10 g / 100 ml which represents 100 grams/liter
Final concentration often expressed as the con in the final volume after mix with CHO and Fat
31. Fat in Parenteral Soln Usually comes in 10% or 20% solutions
10 % represents 1.1 kcal/ml
20 % represents 2.0 kcal/ml
Usually composed of safflower, soy oils with lecithin as an emulsifier to hold in solution
Generally 20 to 30 % of Kcal
Don�t exceed 60% (2.5 g/kg/d)
32. CHO in Parenteral Solution Dextrose monohydrate
D Glucose
Concentrations range from 5% to 70%
Shouldn�t exceed 5 mg/kg/min
Used to spare protein and provide kcals
33. Calculation of Osmolality Dextrose grams/l x 5
Protein grams x 10
Fat is isotonic so no osmotic force
electrolytes further add to osmolarity
50 g of dextrose plus 30 grams of protein
(50 x 5) + (30 x 10) = 550 mOsm/l
34. Indications for Peripheral Vein Feedings 1. Short term: enteral feeding again in 7 d
2. Transition with enteral feeding
3. Mild to mod malnutrition:supplemental nutrition needed
4. Normal or mild elevation of metabolic rate
5. No organ failure or fluid restriction
35. Indications for Central Vein Feeding 1.Unable to enteral feed for 7 + days
2. Mod to severely elevated metabolic rate
3. Moderate to severe malnutrition
4. Cardiac, renal, or hepatic failure or other conditions limiting fluid
5. Limited access to peripheral veins
6. Able to access central vein
36. Compounding Methods Two methods of prescription compounding:
1. All components except fat
2. All components including fat
May be batch mixed to save money
or may be individually prescribed and mixed
Is done by pharmacist in aseptic conditions
37. Administration of TPN Continuous Infusion
Initiate at 42 cc/hr or 1000 L/d
increase incrementally until goal rate is reached over next two to three days
If TPN is interrupted, infuse D10W or D20W until TPN can be restarted
Guard against hypoglycemia
38. Cyclic Infusion To free individuals who are capable of mobility
TPN for 12 to 18 hour infusion periods are possible. Allows pt to be mobile for 6 to 12 hours
Cyclic administration is established incrementally
39. Monitoring and Problem Solving Actual intake of TPN is monitored
Monitor Growth, weight
Metabolic parameters Table 23-7 p549
serum lytes, BG, Hb, etc
General
Volume of infusate, oral intake, urinary output
Infection
Clin Observations: temp., WBC, cultures
40. Refeeding syndrome With intro of energy substrates following a period of no intake, may cause Refeeding Syndrome
Shift of phosphorus, potassium from serum to intracellular sites for ATP production
causes hypophosphatemia, hypokalemia
Can be severe and life threatening
Needs to be monitored and may require additional IV replacement of P and K
41. Transitional Feeding Parenteral to Enteral
begin at 30 cc/hr
increase 25-30 cc/hr every 8 to 24 hours
Parenteral solution is reduced accordingly
Parenteral to Oral
Monitor oral intake; less predictable than above
Reduce Parenteral accordingly
Enteral to Oral
Adjust to intermittent feeding first
42. Nutrition Support in Other Settings Long-term Care
More happening in nursing facilities
Home Care
People are at home receiving nutrition support
Concerns:
motivation
family�s ability to handle
benefit of receiving nut support
limitations such as physical
43. Ethical Issues End of life decisions
Based on advance directives from patient
What is the patient�s desire about end of life support?
Standards and Guidelines
American Society of Parenteral and Enteral Nutrition
Guidelines for use of nutrition support
44. Problems 3 liters of D5W was given via peripheral IV over a 24 hour period. How many kcals did it provide? (1 gram Dextrose monohydrate= 3.4 kcals)
(5 g/100ml) (1000ml/l)(3 l)(3.4 kcal/g)=510 kcal
45. Problem 2.5 l of 3.5% Dextrose
(3.5 g/100ml)(1000ml/l)(2.5 l)(3.4 kcal/g)=
297.5 kcal
46. Problem 3 l of 25% Dextrose and 3.5% Amino Acids
How many kcals and % kcal from each?
(25g/100ml)(1000ml/l)(3 l)(3.4kcal/g)= 2550kcal from CHO
(3.5g/100ml)(1000ml/l)(3 l)(4kcal/g)= 420 kcal from PRO
Total = 2550 + 420 = 2970; 2550/2970=86% from CHO and 14% PRO
47. Problem 500 ml of 10% fat emulsion distributed in 2.5 l of TPN solution which has a final concentration of 20% Dextrose and 3.5 % Amino acids. How many total kcals and what % from each energy nutrient?
(20 g/100ml)(1000ml/l)(2.5 l)(3.4 kcal/g) = 1700 from CHO
(3.5 g/100ml)(1000ml/l)(2.5 l)(4 kcal/g) = 350 from PRO
48. Problem (cont) 10% fat emulsion = (1.1 kcal/ml) (500 ml)= 550 kcal from Fat
Total = 1700 + 350 + 550 = 2600 kcal
1700/2600 = 65% from CHO
350/2600 = 13.4% from Pro
550/2600 = 21 % from Fat
49. Nut Assessment Pt requires 2200 kcal
60% kcal from CHO
25% kcal from fat
15% kcal from PRO
How would you formulate this?
Fat first: you need 2200 x .25 = 550 kcal
10 % fat emulsion @ 1.1 kcal/ml
550 kcal/ 1.1 kcal/ml = 500 ml 10% soln
50. Nut assessment Final volume of 2000 ml
Fat contributes 500 ml
1500 ml for PRO and CHO
2200 kcal x .6 = 1320 kcal/3.4 kcal/g= 388 g CHO/1500 ml = 25 % Dextrose solution
2200 kcal x .15 = 330 kcal/4kcal/g = 82.5 g PRO/1500 = 5.5 % aa solution final concentration