胸腔急症 ~ 氣胸
胸腔急症 ~ 氣胸. 胸腔外科 ~ 黃文傑醫師. 1. 氣胸 ( Pneumothorax): 是氣體在胸腔內引起肺萎陷。若引起縱 隔偏移及壓迫到對側的肺稱之為高張性氣胸 (tension pneumothorax) ,常因使用的人工呼吸器壓力過大而引起,或是 肺氣腫的水泡、肺囊腫破裂而造成。 . 診斷 : i. 理學檢查 : 患側的呼吸音減弱,心音偏向對側。有時頸部有捻 髮音 (crepitus) 。 ii. 胸部 X 光 : 患側呈現高透光性,而且沒有支氣管的顯影。旁邊

胸腔急症 ~ 氣胸
E N D
Presentation Transcript
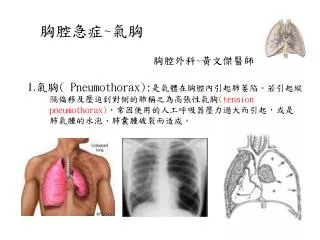
胸腔急症~氣胸 胸腔外科~黃文傑醫師 1.氣胸( Pneumothorax):是氣體在胸腔內引起肺萎陷。若引起縱 隔偏移及壓迫到對側的肺稱之為高張性氣胸(tension pneumothorax),常因使用的人工呼吸器壓力過大而引起,或是 肺氣腫的水泡、肺囊腫破裂而造成。
診斷 : i.理學檢查: 患側的呼吸音減弱,心音偏向對側。有時頸部有捻 髮音(crepitus)。 ii.胸部X光: 患側呈現高透光性,而且沒有支氣管的顯影。旁邊 或甚至對側的肺葉萎陷。縱隔及心臟向對側偏移。 治療 : 無症狀或僅有輕微的呼吸窘迫,可在病房作嚴密的看護,這種 單純性氣胸有三分之二在五至七天內自癒而無須手術。 若有嚴重的呼吸困難及高張性氣胸,則應立即採取行動。以靜 脈注射用之套管針,由前胸第二肋間或腋窩中線第五或第六 肋間插入,接上水下引流瓶,先解除呼吸困難。然後再改用 胸管插入,等肺完全擴張沒漏氣後24-48小時再拔除。 手術(肺氣泡切除術、肋膜沾粘術)
Spontaneous Primary pneumothorax Secondary pneumothorax • Airway and pulmonary disease (COPD, asthma) • Interstitial disease (Pulmonary fibrosis) • Infection ( TB..) • Neoplastic • Catamenial ( Endometriosis) • Iatrogenic • Post-Traumatic
Surgical indication for primary spontaneous pneumothorax • Early complication • Prolonged air leakage • Non re-expansion of the lung • Bilaterality • Hemothorax • Tension • Complete pneumothorax • Potential hazard • Occupational hazard • Absence of medical facilities in isolated areas • Associated single bulla • Psychological • Second Episode • Ipsilateral recurrence • Contralateral recurrence after a first pneumothorax
Spontaneous Pneumothorax-Definition & Factors • Definition Accumulation of intrapleural air as the result of a break in either the visceral or parietal pleura • Factors determining gas reabsorption • Diffusion properties of the gases • Pressure gradients • Area of contact • Permeability of pleural surface
Spontaneous Pneumothorax-Clinical investigation • Signs and symptoms • Sudden onset chest pain • Shortness of breathing • Cough • Diagnosis • CXR • Auscultation • Differential diagnosis • Skin fold • Giant bulla
Treatment Options for Pneumothorax • Observation • Needle aspiration • Percutaneous catheter to drainage • Water seal Pleur-evac type • Heimlich valve • Tube thoracostomy • Water seal Pleur-evac type • Heimlich valve • Tube thoracostomy with instillation of pleural irritant • Video-assisted thoracoscopic surgery • Thoracotomy
Indications for Surgical Intervention • Second episode • Persistent air leakage for greater than 7-10 days • First episode with unexpanded, “trapped” lung • History of contralateral pneumothorax • Bilateral pneumothorax • Occupational risk (driver, airplane pilot, living ina remote area) • Large bulla • Large undrained hemothorax • First episode in a patient with one lung • First episode in a patient with severely compromised pulmonary function
Recurrence of Primary Spontaneous Pneumothorax • Therapy Recurrence (%) • Expectant 30 • Aspiration 20-50 • Chest tube drainage 20-30 • Pleurodesis (tetracycline) 25 • Pleurodesis (talc) 7 • Surgery 2
Complication of Pneumothorax • Tension pneumothorax • Re-expansion pulmonary edema • Persistent air leak • Hemothorax (less than 5%) • Pneumomediastinum
Removal of Chest Tube • Indications • No fluctuation in the fluid column of the tube (complete lung reexpansion or tube occlusion) • Daily fluid drainage <100ml in 24 hours • Air leakage has stopped • Proper timing (controversy) • Spontaneous pneumothorax after tube thoracostomy • removal tube within 6 hours of reexpansion--25% collapse
Tube Thoracostomy ( Chest Intubation)
Indication of Chest Intubation Drain pleural fluid or air promote lung expansion 1. Pneumothorax 2. Hydrothorax 3. Hemothorax 4. Chylothorax 5. Pyothorax 6. Post-thoracotomy etc.
Apparatus of Chest Tube Drainage 1. Underwater sealed bottle: Separate from atmosphere 2. Collecting bottle: Decrease resistance of drainage 3. Negative pressure suction: Promote lung expansion
Procedure of Chest Intubation 1. Local anesthesia, confirm location 2. Skin incision at selected area 3. Dissect into pleural cavity thru a subcutaneous tunnel 4. Deloculate in pleural cavity 5. Insert tube posteriorly and laterally 6. Close incision wound, fixed the tube 7. Connect tube to underwater sealed bottle (or with negative pressure suction)
Attention In Chest Tube Insertion Attention Prevent occurrence 1. Thru thoracostomy wound Underlying organ injury palpate the underlying structure (supra-or infra-diaphragm) 2. Avoid trocar intubation (except Lung or other organ injury emergency) 3. Keep tube in good direction Chest pain, great vessel erosion 4. Avoid intubation thru posterior Pain, unable in supine chest wall 5. Avoid to suture & close Air leakage thoracostomy wound too loose Skin necrosis, pain or too tight
Attention in Massive Subcutaneous (Mediastinal) Emphysema 1. Keep airway patent (even endotracheal tube) 2. CXR 3. Insert chest tube in pneumothorax or suspicious side 4. Connect tube to negative pressure suction immediately 5. Close thoracostomy w’d slightly loose 6. Insert another tube if no improvement 7. Low O2 nasocannula 8. Determine the cause & treat underlying disease 9. Remove tube after complete subsidence
When to Remove Chest Tube ? Criteria: 1. No air leakage 2. Drained fluid < 50 c.c./day 3. Clear serosanguineous color of fluid 4. Full expansion of lung in CXR • Clear sterile fluid remove directly • Turbid, infected fluid withdraw progressively open drain
Attention in Chest Tube Care (I) Attention Prevent occurrence • Fix chest tube firmly Tube moving & contamination • Don’t clamp tube during Tension pneumothorax transportation in presence of air leakage • Don’t use negative pressure suction Abrupt mediastinal shift, after pneumonectomy venous return decrease, death • Don’t apply negative suction Reexpansion pulmonaryedeme immediately after intubation for cases with large volume or long duration of pneumothorax, hydro- pyothorax
Attention in Chest Tube Care (II) Attention Prevent occurrence • Don’t lift up tube above Back flow contamination thoracostomy wound • Use collecting bottle and elevate Back flow contamination the connecting tube between 2 Lung collapse bottles in big residual pleural space or massive air leakage
Attention in Thoracotomy with Lung Resection (I) Attention Prevent occurrence • Suture ligated or close pulmonary Slip out, bleeding vessel with stapler • Make adequate length in bronchial Stump broken stump • Cover bronchial stump with Bronchopleural fistula surrounding tissue, especially in pneumonectomy • Pre-operative anti-TB or anti-fungal Disease flare up drug (at least 2 wks) for suspicious TB or fungal diseases