Download
1 / 25
260 likes | 728 Vues
Gastric and Esophageal Diverticulum Rupture in a Friesian Gelding. Lindsay Chase May 7 th 2014 Clinical advisor: Dr. Kathleen mullen Basic science advisor: dr. Elizabeth buckles. http://tinyurl.com/k4balp7. Signalment and History. 17 year old Friesian Gelding

E N D
Gastric and Esophageal Diverticulum Rupture in a Friesian Gelding Lindsay Chase May 7th 2014 Clinical advisor: Dr. Kathleen mullen Basic science advisor: dr. Elizabeth buckles http://tinyurl.com/k4balp7
Signalment and History • 17 year old Friesian Gelding • 1 day history of inappetence and lethargy • Approximately 8 hour history of colic and dyspnea • rDVM Findings • Tachycardic (80 bpm) • Dyspneic • Febrile (102.60F) • Muddy mucous membranes – CRT 3 seconds • Absent GI motility • Normal rectal palpation
rDVM Therapy • Flunixinmeglumine, detomidine, ceftiofur crystalline free acid • Nasogastric tube • No gastric reflux • Instilled water and mineral oil • Horse became uncomfortable during administration • Referred to Cornell for suspected colitis
Physical Exam • Vital Signs: • T:101.7oF (99-101.5oF) • P: 86 bpm (28-44 bpm) • R: 52 bpm (8-16 bpm) • Depressed • BCS 7/9 • Small amount of malodorous nasal discharge • Cardiovascular • Injected mucous membranes with a toxic line • CRT 3 seconds • Gastrointestinal • Absent gut sounds in all quadrants
Diagnostics • Blood work • PCV: 62% (34-46) • TP: 6.3 g/dL (6.2-7.8) • Hypochloremic metabolic alkalosis • Cl 92 (100-110 mEq/L) • pH 7.523 (7.32-7.44) • BE 8 • HCO3 31 (25-30 mmol/L) • Ionized Hypocalcemia 1.19 (1.25-1.78 mg/dL) • Hyperlactatemia 4.8 (0.3-1.5 mmol/L) • Elevated Creatinine 2.6 (0.4-2.2 mg/dL) • Elevated Troponin 0.68 (0-0.06 ng/mL) • Neutropenia 2.0 (3.0-7.0 thou/uL) • Lymphopenia 1.o (1.8-5.0 thou/uL)
Additional Diagnostics • Thoracic Ultrasound • No pleural fluid or evidence of pleuritis • Abdominal Ultrasound • Stomach of normal size • Thickened large colon and small intestinal walls • Imaging was difficult because of BCS • No appreciable peritoneal fluid • Rectal Exam • Thickened but compressible loops of small intestine • Nasogastric Intubation • Unable to pass tube beyond the cardia
Problem List Colic Thickened SI and colon Inability to pass NG tube into stomach Tachypnea Endotoxemia Dehydration Hypoproteinemia Hypochloremic metabolic alkalosis Hypocalcemia Hyperlactatemia Leukopenia http://pad2.whstatic.com/images/b/ba/Sickhorse.jpg
Initial Stabilization and Treatment 1L Hypertonic saline bolus 20L Plasmalyte bolus Plasmalyte CRI with electrolyte supplementation Hetastarch CRI Lidocaine CRI Antiendotoxic dose of flunixin (0.25 mg/kg) Cryotherapy Offered 3L of water – after drinking became uncomfortable Photo courtesy of Dr. Sally Ness
Re-evaluation • No clinical improvement • Thoracic ultrasound • Pleural fluid • Abdominal ultrasound • Copious amounts of flocculant peritoneal fluid • Upper GI Endoscopy • Impaction of feed material in distal esophagus • Abdominocentesis • Septic peritonitis consistent with GI rupture • Euthanasia was elected and a necropsy was performed Photo courtesy of Dr. Sally Ness Photo courtesy of Dr. Katie Mullen
Gross Findings Peritoneal cavity contained ~60 L of peritoneal effusion with copious amounts of fibrin. No feed material was found in the fluid. Photo courtesy of Dr. Kim Bonner
Gross Findings Left: 8 cm tear in impacted esophageal pulsion diverticulum caudal to the diaphragm Right: Severe smooth muscle hypertrophy of caudal esophageal wall (1.7 cm (normal thickness 0.5 +- 0.1 cm)) Photos courtesy of Dr. Kim Bonner
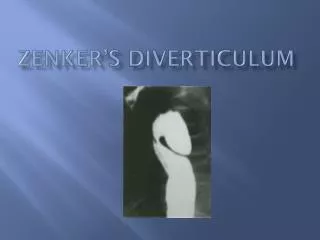
Esophageal Diverticula • Types of Diverticula • Traction • Shallow body and wide opening • Usually secondary to esophageal injury • Able to transmit peristalsis • Not prone to impaction • Pulsion • Flask-like body and narrow opening • Mucosa protrudes through a defect in esophageal wall • Prone to impaction • Usually located in cervical region in the horse
Gross Findings Left: Full thickness gastric tear (5.5 cm) located within a 10 cm partial tear (separation of tunica muscularis) along the lesser curvature Right: Severe edema in pyloric gastric wall Photos courtesy of Dr. Kim Bonner
Regional Anatomy Esophagus Stomach Diaphragm Liver Left Dorsal Colon Left Ventral Colon 3 1 2 4 5 6 Color Atlas of Veterinary Anatomy, Volume 2, The Horse. Vol. 2: Elsevier Health Sciences, 2012. 160. Print.
Histopathology • Distal Esophagus • Thickened tunica muscularis • No underlying condition was found that would have predisposed to either the gastric or esophageal lesions Photo courtesy of Dr. Elizabeth Buckles
History of the Breed 1500-1600 - Developed in the Friesland province of the Netherlands 1879 – Studbook was founded 1913 – Only 3 approved stallions 1928 – 8 approved stallions bred 358 mares Currently 45,000 registered Friesians http://tinyurl.com/lcyvxcl http://tinyurl.com/ophacvb
Common Anomalies and Diseases Dwarfism Hydrocephalus Retained placenta Chronic Proliferating Lymphangitis Megaesophagus Aortic rupture Aortopulmonary fistulas All photographs: Boerma, S., W. Back, and M. M. Sloet Van Oldruitenborgh-Oosterbaan. "The Friesian Horse Breed: A Clinical Challenge to the Equine Veterinarian?" Equine Veterinary Education 24.2 (2012): 66-71. Web.
Current Research • Retrospective study conducted in 2013 • 852 horse necropsies over 6 years at Michigan State University • 42 horses had gross esophageal lesions, 10 were severe • 35.3% of Friesians submitted had severe esophageal lesions compared to 0.5% of other breeds • Most common lesion was caudal esophageal smooth muscle hypertropy • Prevalence in Friesians: 35% and all other breeds <3% • Usually an incidental idiopathic finding in older horses • Megaesophagus was present in 6 Friesian horses, 5/6 had severe muscular hypertrophy
Current Research • Aortic Rupture • Study published in April 2014 showed specific histological changes • Accumulation of mucoid material • Disorganization and fragmentation of elastic laminae • Smooth muscle hypertrophy • Medial necrosis • Hypothesized to be a genetic connective tissue disorder of elastin or collagen • Dwarfism • Tendons of dwarf Friesians and non-dwarf Friesians have been shown to have more elastic properties compared to control ponies
Fenway Foundation for Friesian Horses • Mission Statement • “The Fenway Foundation for Friesian Horses is a not for profit corporation created to preserve and enhance the longevity and quality of life of Friesian horses by accruing pertinent equine, more specifically Friesian, information to educate the public and offering assistance regarding Friesian horses and their owners throughout North America.” • Services • Rescue assistance • Necropsy assistance • Health assistance • Genetic assistance • Educational assistance • Continuing Care Assistance Upon Incapacitation Or Death http://www.fenwayfoundation.com/index.html
Necropsy Assistance • The foundation will reimburse for necropsies on Friesians 17 years old and younger • Work in conjunction with Dr. Back at Utrecht University on the following: • Hydrocephalus • Dwarfism • Aortic rupture • Megaesophagus • Detailed necropsy guidelines and sample information found at: • http://www.fenwayfoundation.com/services.html
Final Cost • Emergency Colic Work-up • $768 • Medications, Fluids and Supplies • $852.23 • Diagnostics • $393.19 • Necropsy • $214.40 • Total: $2227.82 • - Reimbursement from Fenway Foundation http://www.kimballstock.com/pix/HOR/01/HOR_01_MB0134_01_P.JPG
References Benders, N. A., J. B. VeldhuisKroeze, and J. H. Van Der Kolk. "Idiopathic Muscular Hypertrophy of the Oesophagus in the Horse: A Retrospective Study of 31 Cases." Equine Veterinary Journal 36.1 (2004): 46-50. Web. Boerma, S., W. Back, and M. M. Sloet Van Oldruitenborgh-Oosterbaan. "The Friesian Horse Breed: A Clinical Challenge to the Equine Veterinarian?" Equine Veterinary Education 24.2 (2012): 66-71. Web. Fenway Foundation for Friesian Horses. N.p., n.d. Web. <http://www.fenwayfoundation.com/index.html>. "Friesian Timeline." Friesian Horse Association of North America. N.p., 2014. Web. 01 May 2014. <http://www.fhana.com/timeline/>. Komine, M., I. M. Langohr, and M. Kiupel. "Megaesophagus in Friesian Horses Associated With Muscular Hypertrophy of the Caudal Esophagus." Veterinary Pathology Online (2013): n. pag. Sage Publications. Web. 1 Apr. 2014. <http://vet.sagepub.com/content/early/2013/11/13/0300985813511126>. Ploeg, M., V. Saey, C. Delesalle, et. al. "Thoracic Aortic Rupture and AortopulmonaryFistulationin the Friesian Horse: Histomorphologic Characterization." Veterinary Pathology Online (2014): n. pag. Sage Publications. Web. 25 Apr. 2014. <http://vet.sagepub.com/content/early/2014/04/16/0300985814528219>. Yamout, S. Z., K. G. Magdesian, and D. A. Tokarz. "IntrathoracicPulsion Diverticulum in a Horse." Canadian Veterinary Journal 53 (2012): 408-11. Web.
Questions? • Thank you to: • My advisors • Dr. Buckles • Dr. Mullen • Class of 2014! http://animals.desktopnexus.com/wallpaper/533523/