Malignancy
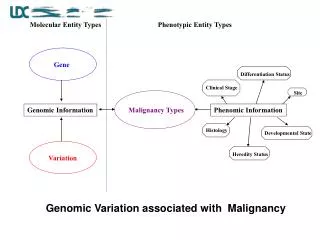
Malignancy. Acute lymphoblastic leukemia Failure of the cell maturation. Immunological classification. Common ALL: (~75%) Defined by the presence of CD10. Phenotypically pre-B (ie the cells carry the same surface antigen as the pre-B lymphocyte). Any age may be affected, commonly 2 -4 yr-olds.

Malignancy
E N D
Presentation Transcript
Immunological classification • Common ALL: (~75%) Defined by the presence of CD10. Phenotypically pre-B (ie the cells carry the same surface antigen as the pre-B lymphocyte). Any age may be affected, commonly 2 -4 yr-olds. • T-cell ALL: Any age but peak in adolescent males, eg presenting with a mediastinal mass and a high WCC. • B-cell ALL (Burkitt or Burkitt-like leukaemia): Rare. Bad prognosis. Immunoglobulins present on blast cells. • Null-cell ALL: Undifferentiated, lacking specific markers above.
Morphological classification • The FAB system (French, American, British) divides ALL into 3 types • (L1, L2, L3) by microscopic appearance. Although widely used, it provides only limited information compared with other systems • L1 –lymphoblast is the most common in children (80-85%) has scanty cytoplasm and inconspicuous nucleoli. L1 is associated with better prognosis. • L3 is morphological similar to Burkitt’s lymphoma
Acute lymphoblastic leukemia. The cells are heterogeneous in size, have round or convoluted nuclei, high nuclear/cytoplasmic ratio, and absence of cytoplasmic granules.
Treatment • Specific chemotherapy:4 steps The aim is destroy the leukemic clone cells • Remission induction: 4 to 6 wks -vincristine 1.5 mg/m square iv weekly -prednisolone 40 mg/m square orally daily. -L-asparaginase 6000ug/m sq. iv daily for 14 days.
CNS prophylaxis(intra thecal) -methotrexate 15 mg/m sq. -hydrocortisone 15 mg/m sq. -cytosine arabinoside 30 mg/m sq. weekly for 6 weeks during induction then 8 wkly for 3 yrs. • Consolidation (reinforcement therapy): --vincristine 1.5 mg/m sq. iv 8 weeks --prednisolone 40 mg /m sq. /day orally 28 days every 16 week.
Mantainance therapy( 2- 3 yrs) -6-mercaptopurine 50mg/m sq./day orally. -methotrexate 20 mg/m sq./week orally. -relapse is common in blood ,CNS and testis.
Supportive treatment • Anemia : packed cell or whole blood transfusion to maintain Hb above 10 gm/dl. • Bleeding : platelets or whole blood transfusion to maintain platelets count above 1 lac/ mm cub. • Infection : broad sepctrum antibiotics.
Bone marrow transplantation :allogenic or autologous bone marrow trasplantation is considered if poor prognosis.
ACUTE MYELOID LEUKEMIA • This neoplastic proliferation of blast cells is derived from marrow myeloid elements. It is a very rapidly progressive malignancy (death in ~2 months if untreated; ~20% 3-yr survival after chemotherapy).
Incidence • 1/10,000/yr. Increases with age, and is the commonest acute leukaemia of adults. Seen increasingly as a long-term complication of chemotherapy, eg for lymphoma. Also associated with ionising radiation and syndromes eg Down's.
Classification • AML can be divided into several groups according to FAB morphological classification: • M0- immature • M1- acute myeloblastic leukemia with minimal maturation • M2- acute myeloblastic leukemia with maturation • M3-acute promyelocytic leukemia • M4 –acute myelomonocytic leukemia • M5-acute monoblastic leukemia • M6-erythroblastic leukemia • M7-acute megakaryoblastic leukemia
About 30 to 40% of case of AML are M1 and M2 and abt same percentage are M4 and M5. • M3 type of AML constitutes about 5-10%. • M7 (megakaryoblastic leukemia) is strongly associated with down syndrome.
Symptoms • Marrow failure: Patients usually present with symptoms of anaemia, infection or bleeding. DIC occurs in acute promyelocytic leukaemia, a subtype of AML (M3), where there is release of thromboplastin. • Infiltration: Hepato- and splenomegaly, gum hypertrophy, skin involvement. • CNS involvement at presentation is rare in AML.
Chloromas (also called granulocyte sarcoma) are localized collection of leukemic cells seen almost exclusively in patients with AML. • They may occur at any site including CNS ,bones (typically orbit ) and skin . • Gingival hypertrophy may be present.
Diagnosis • WCC is variable, but can be normal or even low. • Blast cells may be few in the peripheral blood, so diagnosis depends on bone marrow biopsy. • Differentiation from ALL may be by microscopy (Auer rods are diagnostic of AML), but is now based on immunophenotyping and molecular methods. • Cytogenetic analysis (eg type of mutation)
Complications • Infection is the major problem, related to both the disease and during treatment. • Should be alert to septicaemia . Infections may be bacterial, fungal or viral, and prophylaxis is given for each during treatment. • Chemotherapy causes increase plasma urate levels (from tumour lysis) so give allopurinol with chemotherapy, and keep well hydrated with IV fluids.
Treatment • Supportive care • Chemotherapy is very intensive, resulting in long periods of marrow suppression with neutropenia + thrombocytopenia. The main drugs used include daunorubicin, and cytosine arabinoside, with ~5 cycles given in 1 week blocks to achieve remission.
Bone marrow transplant (BMT) • Pluripotent haematopoietic stem cells are collected from the bone marrow. • Allogeneic transplants from HLA-matched siblings • Destroy leukaemic cells and the immune system by cyclophosphamide + total body irradiation, and then repopulate the marrow by transplantation from a matched donor infused IV. • Ciclosporin and methotrexate may be used to reduce the effect of the new marrow attacking the patient's body
Complications: Graft vs host disease; opportunistic infections; relapse of leukaemia; infertility. • Autologous BMT where stem cells are taken from the patient themselves, is used in intermediate prognosis disease