Download
1 / 28

E N D
1. Post operative Pain and Regional Anaesthesia Dr Maya Nagaratnam FFPMRCA FRCA
3. Why is it important to control pain? Divinum sedare dolorem
Reduce Sympathetic activity ( ACS)
Reduce respiratory complications
Reduced chronic pain syndromes
Improved mobilisation
Improved patient satisfaction
4. Divinum sedare dolorem
5. Reduce respiratory complications
6. Reduce Sympathetic activity ( ACS)
7. Improved mobilisation
8. Reduce Chronic Pain Syndromes
9. Improved patient satisfaction
10. Case 1 It is your first on call as a Gas person.
Bleeped about Mrs X
DSU laproscopic cholesystectomy;
admitted overnight for uncontrolled pain.
PONV
11. Put the following in the right order A. d/w Spr
B. management plan
C. history and pain assessment
D. check notes, anaesthetic and drug charts
12. D, C, B ,A D. check notes, anaesthetic and drug charts
C. history and pain assessment
B. management plan
A. d/w Spr
13. Pain Assessment
14. Management Options A. regular oral analgesia eg paracetamol, diclofenac, prn Im morphine
B. regular IV paracetamol, prn IM morph, IVF, antiemetic
C. morphine PCA
D.Immediate IV morphine 0.5-1mg/kg titrate in 2mg aliquots
E. C +D+ IVF+ antiemetic.
15. WHO analgesic ladder....1, 2, 3
16. Analgesia Simple(mild)
Paracetamol
NSAIDs Moderate
Codeine
Tramadol
17. General points Ladder -Breakthrough pain - strong analgesics as per WHO pain ladder
Oral -Regular oral analgesia ASAP
Others -Treat co existing symptoms; fluids, antiemetic, laxatives , oxygen
18. CASE 2 57 y old 3d post laporotomy, thoracic epidural, can take free fluids
Excruciating pain last 2 h A. Morphine PCA
B. Notes, drug chart
C. D/W SpR
D. Hx, examination ( epidural site)
E. Regular oral analgesia, breakthrough morphine
F.Bolus/ top up
19. B, D, F, E, A, C B. Notes, drug chart
D. Hx, examination ( epidural site)
F. Bolus/ top up
E. Regular oral analgesia, breakthrough morphine
A. Morphine PCA
C. D/W SpR
20. Regional analgesia Peripheral nerve block
Mainly extremeties, particularly ortho
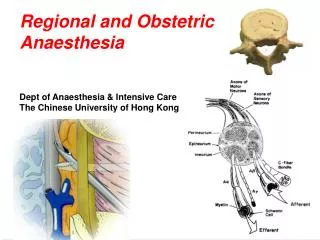
Epidural
Used as both analgesia and anaesthetic, usually catheter in situ can top up
Spinal
Similar to epidural , but lower concentrations required, rarely catheter in situ, continuous prolonged analgesia not appropriate
21. Peripheral Nerve Block
22. Spinal (A) v Epidural (B)
23. Summary � control of POP
24. General concepts pain treatment L
O
O
25. General concepts pain treatment L (ladder) � WHO pain ladder ; stepwise increment of strength of analgesia; start at appropriate level
O (oral) establish oral analgesics ASAP
O (other assoc. symptoms ) Treat N, V, dehydration, constipation, anxiety.
27. Learning Objectives List 6 important reasons for post operative pain control
Choose appropriate analgesic regimes
Know when to call for senior advice