Download
1 / 29
330 likes | 888 Vues
TRAUMA OF THE CHEST. A. VAYDA department of surgery with anesthesiology. Classification The closed damages of the chest are divided: І. According to the injury of other organs: 1.Isolated trauma. 2.Combined trauma (craniocerebral, with damage of abdominal organs, with damage of bones).

E N D
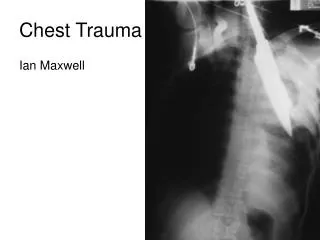
TRAUMA OF THE CHEST A. VAYDA department of surgery with anesthesiology
Classification • The closed damages of the chest are divided: • І. According to the injury of other organs: • 1.Isolated trauma. • 2.Combined trauma (craniocerebral, with damage of abdominal organs, with damage of bones). • II. According to the character of complications: • 1.Uncomplicated. • 2.Complications: • Early (pneumothorax, hemothorax, mediastinal emphysema, flail chest, traumatic shock, asphyxia); • Late (posttraumatic pneumonia, posttraumatic pleurisy, suppurative diseases of lungs and pleura).
Rib fracture • The direct force of traumatizing factor on the chest wall results in rib fracture. • Pain • On examination the respiratory lag on affected side. • Crepitating of osseous fragment revealed by palpation diminished breathing sounds by auscultation depending on number of injured ribs • On chest roentgenograms the break in continuity of bone fragments of ribs is observed.
Floating rib fracture (Flail chest) • The floatation arises from fracture of three and more ribs along two anatomic lines. The multiple rib fractures produce an unstable segment of chest wall that moves paradoxically inward upon inspiration and balloons outward during expiration (flail chest). Thereby the respiration disturbed not only in the area of a floatating segment, but also in all lungs. The permanent movement of floatating segment result in rocking shift of mediastinum, which causes deviation of its organs. As a result the respiratory failure is associated with cardiovascular.
Treatment • Pain relief in closed trauma of the chest is achieved by means of different blocks: • Vagosympathetic block; • Alcohol - novocaine block of the site of fracture; • Paravertebral block. • Analgesics and opiates. • The methods of reduction of the skeleton of the flail chest are divided onto three groups: • External fixation of a movable segment by means of suturing for intercostal muscles and traction during 2-3 weeks • Intrmedullary costal osteosynthesis; • Mechanical ventilation (often with positive end-expiratory pressure).
Posttraumatic pneumothorax Posttraumatic pneumothorax is the presence of air in a pleural space, caused by mechanical injury of lung or chest wall as a result of trauma.
Classification • І. According to extension of process: • Unilateral. • Bilateral. • ІІ. According to degree of a lung collapse: • Partial (collapse of lung to 1/3 of its volume). • Subtotal (collapse of lung to 2/3 of its volume). • Total (collapse of lung exceeding 2/3 of its volume). • ІІІ. According to the mechanism of occurrence: • Closed. • Open. • Valvular.
Symptomatology and clinical course • The rest dyspnea. • The chest pain. • By percussion obtains bandbox sound, or tympanitis. • By auscultation - weak or absent breathing sounds. • Lag on affected side. • On the background of severe trauma of the chest the signs of damage dominate in clinical manifestation on inappreciable entry of air in a pleural space. • Pneumothorax mostly revealed during X-ray examination.
Treatment • Aspiration of air by means of thoracentesis, closed drainage of a pleural space. • The absence of effect (incomplete expansion of lung) of active aspiration, and also valvular closed pneumothorax is the indications to operative management – suturing of the pulmonary wound
Hemothorax Hemothorax is the accumulation of blood in a pleural space. The cause of occurrence of this complication is the damage of vessels of the chest wall, pleura, lungs and mediastinum.
Classification • І. According to degree of hemorrhage: • Small (the loss less 10 % of volume of circulating blood). • Moderate (loss of 10-20 % of volume of circulating blood). • Great (loss of 20-40 % of volume of circulating blood). • Total (exceeds 40 % of volume of circulating blood). • ІІ. According to duration of bleeding: • With continuing hemorrhage. • With the stopped bleeding. • ІII. According to the presence of clots in a pleural space: • Coagulated. • Noncoagulated.
Symptomatology and clinical course • If hemothorax is the complication of blunt chest trauma, the clinical manifestations depend on the gravity of trauma and degree of hemorrhage. Also hemothorax by itself results in pulmonary compression and shift of mediastinum. • In case of small hemothorax clinical manifestations of hemorrhage are slightly expressed or absent at all. • Dyspnea, cough, general malaise and dizziness are obvious in moderate hemothorax. The skin is pale. The hemodynamic disturbances – tachycardia and decreased arterial pressure are observed. • The great and total hemothorax are associated with signs of shock. • By percussion the dullness is revealed. • By auscultation - the breathing over the site of hemothorax is sharply diminished or is not heard.
On X-ray picture of hemothorax the intensive homogeneous shadow on the side of the lesion with oblique upper contour is observed. The costal sinus does not visualized. • In small hemothorax, depending on the degree of intrapleural bleeding, the shadow observed only in the region of sinus. • In moderate hemothorax it achieves a scapular angle (on the back surface) or V rib on anterior surface of the chest wall. • In great hemothorax this shadow achieves ІІІ rib, and total hemothorax characterized by complete shadow of a pleural space.
Treatment • A treatment of small hemothorax requires needle aspiration or drainage of pleural space and elimination of blood. The manipulation is carried out in VІ-VІІ intercostal spaces in the postaxillary or scapular lines. • Total, great or moderate hemothorax with persistent bleeding (positive test by Revilour-Greguar) requires thoracotomy for liquidation of a bleeding source. • The bleeding wounds of lungs are sewed up by twist suture. If the pleural space contains liquid blood, the surgeon carries out its reinfusion. The clots are removed from pleural space.
Mediastinal emphysema • Mediastinal emphysema is the complication of the blunt trauma of the chest, which is characterized by entering and accumulation of air in mediastinum. The entry of air in mediastinum leads to compressing of superior cava vein and right atrium, which results in the expressed discirculation. • The causes of mediastinal emphysema is partial (damage of a membranous part) or complete disruptions of trachea, bronchi, esophagus and in some cases – tension pneumothorax.
Symptomatology and clinical course • Difficult breathing and swallowing. • Pain behind breastbone. • Hoarseness. • Cough attacks. • The neck and face are thickened, cervical veins distended, the skin is cyanotic. • By palpation – the crepitation of neck, face, and shoulder area. • On X-ray film on the background of enlightenment observed well-defined contour of a mediastinal pleura.
Tactics and choice of treatment Progressing mediastinal emphysema requires the urgent drainage of anterior mediastinum in order to prevent external cardiac tamponade.