Download
1 / 19
190 likes | 289 Vues
Whole system improvement in Forth Valley. Improvement and support team meeting 15 th Jan 2009. Context. Period of significant change and innovation National collaborative projects Integrated healthcare strategy includes new acute hospital 2010-2011 Consistent bed pressures

E N D
Whole system improvement in Forth Valley Improvement and support team meeting 15th Jan 2009
Context • Period of significant change and innovation • National collaborative projects • Integrated healthcare strategy includes new acute hospital 2010-2011 • Consistent bed pressures • Need for step change in results from improvement activity • Implementation • Measureable benefit • Focus and prioritisation
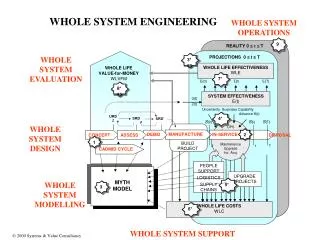
Cycle Time (CT) Resources (R) = Takt Time (TT) Lean improvement • It’s about BALANCE and FLOW
Improvement on the ‘shop floor’ Failure Count Failure Reason 1 Failure Reason 2 Failure Reason 3 Failure Reason 4 Failure Reason 5 Failure Reason 6 # Who When Status Action ü 1 ~~~~~~~~~~~~ ~~~~ ~~/~~/08 2 ~~~~~~~~~~~~ ~~~~ ~~/~~/08 ü 3 ~~~~~~~~~~~~ ~~~~ ~~/~~/08 4 ~~~~~~~~~~~~ ~~~~ ~~/~~/08 1. Measure actual v target for key processes 2. Assign reasons for process failure, and count … Target Process performance time 3. Routinely act on the most costly failures using: Concern Cause Countermeasure Multi-disciplinary team, according to problem
Process 20th Oct start 2&3 Dec 17&18 Dec 12th Nov Phase 1 Phase 2 Phase 3 Phase 4 Phase 5 Phase 6 Prioritisation Event Policy & Planning Event Analyse the Forth Valley Whole System Top Team Event Analyse Priority Areas Evaluate Options 2 - 4 weeks 1 day 1 - 2 weeks 1-2 days 1 - 2 weeks 2 days
Executive challenge • Transition to new models of care across system • £14.5m - £25m savings by Mar 2011 • Maximum 18 week RTT by Dec 2011 • Resilient U&E flow = 98% A&E asap • Consistent, safe care: • HAI down by 30% by 2010
Specialist acute care tertiary services Community Pharmacists Clinic Day Patient In Patient GP Home Visit mental health; elderly care GDP district nursing health visiting Local Authorities Optom specialist nursing AHP (e.g. physio, OT) family health services Partner & Vol organisations other community services – partnership model with LA Forth Valley System Map NHS 24 OOH SAS MIU OOH, urgent & emergency services (community) A&E amb care in-patient refer to GP CAU acute receiving unit GP referral routine discharge rehab out-patient GP referral GP feedback AHP (physio) day case diagnostics complex discharge GP direct access acute services sub-contract out-reach refer on-going community care GP referral GP direct access
166,000 - NHS 24 OOH 25,100 SAS MIU 52,600 OOH, urgent & emergency A&E services (community) amb care Specialist acute care refer to GP 26,000 LOS=6.8 GP CAU tertiary services referral 12,000 acute 27,500 M 4,300 routine in - patient receiving discharge unit GP out - patient referral 41,000 LOS=3.8 196,000 9,600 GP rehab feedback AHP ( physio ) GP diagnostics day case complex direct discharge access 13,500 acute services sub - contract out - reach 50,000 refer on - going community care Community 80% occ ; Pharmacists 294 beds 1,300,000 Clinic Home Visit Day Patient In Patient GP GP mental health; elderly care referral GDP district nursing 300,000 65,000 health visiting ~130,000 Local Optom 32,000 specialist nursing GP Authorities 81,000 AHP direct (e.g. physio , OT) family health services access 962,000 Partner & Vol other organisations community services – partnership model with LA 789k OP; 135k IP 7 Forth Valley Planning Event Forth Valley System Map
Specialist acute care tertiary services Community Pharmacists Clinic Day Patient In Patient GP Home Visit mental health; elderly care GDP district nursing health visiting Local Authorities Optom specialist nursing AHP (e.g. physio, OT) family health services Partner & Vol organisations other community services – partnership model with LA 166,000 Forth Valley System Map NHS 24 OOH 25,100 SAS MIU +1.1% 52,600 OOH, urgent & emergency services (community) A&E amb care in-patient +2% refer to GP CAU 26,000 LOS=6.8 acute receiving unit GP referral 38,000 12,000 routine discharge rehab 27,500 M 4,300 out-patient GP referral 41,000 LOS=3.8 196,000 9,600 GP feedback -26% +24% (new) AHP (physio) diagnostics day case complex discharge GP direct access 13,500 3,000 acute services +3% sub-contract out-reach 50,000 refer on-going community care +12% 330k AHP 32k Nr 28k DP; 17k OP 80% occ; 294 beds +5% 1,300,000 GP referral 300,000 65,000 ~130,000 32,000 GP direct access 81,000 963,000
Specialist acute care tertiary services Solutions to imbalance lie in whole system … NHS 24 OOH T SAS MIU T OOH, urgent & emergency services (community) A&E amb care in-patient refer to GP CAU acute receiving unit GP referral routine discharge rehab Q out-patient GP referral GP feedback Q Q Q AHP (physio) diagnostics day case complex discharge GP direct access acute services sub-contract out-reach refer on-going community care Community Pharmacists Clinic Day Patient In Patient GP Home Visit GP referral mental health; elderly care Q GDP district nursing health visiting Local Authorities Optom specialist nursing GP direct access AHP (e.g. physio, OT) family health services Partner & Vol organisations other community services – partnership model with LA
1st OP Appt Outcome Discharged 24.8%DNA 4%Failed Discharge 1.7%Awaiting Results 8.8%Waiting List DC 4%Ref other Clinics 2.7%IP wtg list 7%Blank/Other 8.8%Further Appt 38.4% Losses = 29% of capacity Outpatients Scheduled capacity 80% of demand Demand 1000Capacity 793 23.4 wks 45 wks (83% > 18 wks) Quality Losses 17-42% 3.2 Planned Orthopaedics Outpatients OP – Lost Capacity Hips – Sept 08Capacity 363Pts seen 255(overtime 69)DNA 13Unfilled Appt 44Canc Clinic 50 home Pre-Op Theatre in-patient Discharge out-patient out-patient GP referral refer on-going community care day case diagnostics 9.5 wks 16.5 wks
Discharges by day of the week Approx 60 bed days a week (£1.6M p.a.) 19% Sunday shortfall
Distribution of acute LOS Avoid admission and ambulatory care … Are there 3 themes here ? Reduce LOS by improved inpatient and discharge processes Generally elderly patients. Avoid admission …
District nurse diary study:conclusions • Opportunities to increase productivity • Reducing lost time (eg. admin, meetings etc) • Scheduling domiciliary time more efficiently • Using lower grade staff for routine work • Shifting routine treatment room work to GP practices and phlebotomist • Improving predictive planning with acute services • Balancing nursing resource effectively to meet 7 day a week demand • Opportunities for released capacity • Increased capacity in treatment rooms to support acute discharge • Increased capacity for anticipatory care • Understanding return on investment of different options
NHS Forth Valley Priority Improvement Work-Streams Elective Work-stream Urgent & Emergency Work-stream Primary & Community Work-stream Reduce variation in referral management Redesign whole system U&E pathway Releasing/developing capacity in primary care and community services Mainstream advanced care planning to reduce inappropriate hospital admissions Systematic improvement in LA supported discharge Improve ‘home-to-home’ visibility of patient pathway Improve quality of Urgent and Emergency “front door” services Diagnostics Work-stream Systematic improvement of Labs Increase CT (MRI) productivity / capacity Reduce avoidable unplanned admissions Articulate the productivity benefits from 18 week programme Systematic improvement in acute in-patient management Enabling Work-streams : Leadership & Communication; Information & Metrics; Training; Programme Mgt;
Conclusions • Whole system perspective was revealing • Increased focus on primary and community care • Process highlighted the need for good information • Real focus on evidence • Challenged us about how we prioritise resource use • Produced plans with clarity and shared understanding