Download
1 / 82
1.36k likes | 2.61k Vues
Basic Fetal Monitoring. Southwest Washington Perinatal Education Consortium. Kathleen Murray, CNM, MN, RN. Objectives. Identify the components of a fetal heart rate pattern: baseline, variability, accelerations, decelerations, periodic, and non-periodic changes

E N D
Basic Fetal Monitoring Southwest Washington Perinatal Education Consortium Kathleen Murray, CNM, MN, RN
Objectives • Identify the components of a fetal heart rate pattern: baseline, variability, accelerations, decelerations, periodic, and non-periodic changes • Discuss maternal and fetal physiology and how it influences fetal heart rate patterns • Differentiate criteria for reassuring and non-reassuring fetal heart rate patterns
Fetal Heart Rate Monitoring Techniques • Auscultation • Fetoscope
Auscultation • Fetoscope Low tech Need quiet room
Auscultation • Doppler Motion detector Portable Some models are made for underwater use (in tub)
Doppler Doppler used throughout pregnancy and labor
Auscultation Benefits • Detects baseline • FHR rhythm and dysrhythmias • Hear changes in fetal heart rate • Differentiates maternal from fetal heart rate
Auscultation Limitations • Not continuous • No printout or computer record • Can’t demonstrate variability • Requires some 1:1 nurse-time • May be limited by position of mother
Fetal Heart Rate Monitoring Techniques • Electronic Fetal Monitoring External Internal
What’s thePurposeof FetalMonitoring???
Purpose of Electronic Fetal Monitoring • Identify reassuring signs of fetal well-being • Screen for non-reassuring signs of a fetus who is at risk
Benefits of External Fetal Monitoring (EFM) • Noninvasive • Paper document • Demonstrates variability • Less labor intensive
Limitations of EFM • Restricts patient movement • Measures cardiac motion, is not ECG • Doubling or half-count of FHR possible • Might pick up maternal HR instead
Internal Fetal Monitoring • Spiral electrode (FSE) provides direct ECG • Measures interval between R waves • Produces very accurate picture of FHR
Benefits of Internal Monitoring (Using FSE) • Accurate measure of FHR and variability • May detect dysrhythmias • Can allow for more patient movement
Limitations of FSE • Membranes must be ruptured to use • Risk of infection • If fetus has died, may pick up maternal heart rate accidentally
Uterine Activity Monitoring • External: tocotransducer • Detects frequency and length, not strength • Requires palpation to assess strength of contractions
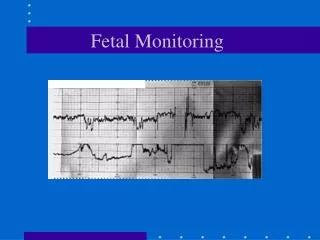
Uterine Monitoring • Note the normal-looking UC first • Then baseline rises and next few UC’s seem high (false) • External UC monitor does not accurately show strength
BENEFITS Noninvasive Provides documentation of UC frequency and duration LIMITATIONS Does not measure strength of contraction, nor resting tone of uterus Difficult to use in maternal obesity, in some positions External Uterine Monitoring
Monitoring With Internal Uterine Pressure Catheter (IUPC) • Accurate measure of uterine pressure • Contraction strength, and resting tone • Measured in mmHg • Accurate timing of FHR changes in relation to UC’s
INDICATIONS External reading not adequate Labor dystocia Fetal distress Amnioinfusion for cord compression RISKS Infection Uterine perforation Placental injury Extraovular placement IUPC
Fetal Heart Rate Monitoring • Baseline, rounded up to nearest 5 bpm • Variability • Accels and Decels • Periodic changes (with UC’s) • Non-periodic changes (spontaneous)
Fetal Heart Rate Monitoring • Baseline • Normal: 110-160 bpm • Tachycardia : >160 bpm for >10 minutes • Bradycardia: <110 bpm for >10 minutes
Variability • Characteristic of FHR baseline • Smoothness, or roughness of the line • Very important characteristic of FHR, must be present for reassuring strip
Variability • Assessed in between UC’s and periodic changes • Absent: undetectable • Minimal: 1-5 bpm amplitude • Moderate: 6-25 bpm (normal) • Marked: >25 bpm (also called saltatory)
Non hypoxic causes Fetal sleep (20 min) Medications Tachycardia (such as from maternal fever) Fetal anomaly dysrhythmia Hypoxic causes Uteroplacental insufficiency Cord compression Mat. Hypotension Tachysystole Abruption Tachycardia Causes of Decreased Variability
Interventions • Determine cause • Position change • IV fluids • Oxygen 10 liters snug face mask • Stop or turn down pitocin • Place internal FSE • Notify MD/CNM without delay
Sinusoidal Pattern • Not to be confused with variability!! • Regular, sine-like wave pattern with amplitude of 5-15 bpm above and below baseline • Ominous in most cases, requires prompt intervention, usually immediate C-section • Usually caused by severe fetal anemia, can be from hypoxia, or briefly from narcotic dose
Causes of Increased Variability • Uteroplacental insufficiency or • Cord Compression or • Fetal Activity and • A compensatory response to a mild hypoxic event
Interventions • Determine cause • Position change • Assess fetal response
Accelerations • Caused by sympathetic nervous system response to fetal movement or stimuli, normal and reassuring, rules out acidosis • But, periodic accels, with UC’s are mild cord compression
Criteria for Accelerations • <32 weeks gestation, stays 10 beats above baseline for at least 10 seconds • For > 32 weeks, acceleration stays 15 beats above baseline for at least 15 seconds
Early Decelerations • Caused by pressure on fetal head, vagal response • Uniform, mirrors contraction • Gradual onset, reaches nadir >30 sec. • Reaches nadir at peak of UC, returns to baseline by the end of UC • Benign
Variable Decelerations • Caused by cord compression, baroceptor response quickly slows FHR to compensate • Abrupt onset, reaches nadir < 30 sec. • Decel. Of >15 bpm lasting > 15 sec., and return to baseline < 2 minutes
Intrauterine Nuchal cord, or body entanglement Oligohydramnios Rupture of membranes Short cord or true knot Occult prolapse of cord Maternal conditions Positioning Second stage labor with descent Monoamniotic multiple gestation Causes of Variable Decelerations