Download
1 / 1
10 likes | 215 Vues
Poster Number: B13. FDA Office of Women’s Health Funded Pregnancy and Lactation Related Studies: 2001 – 2008 Omolara R Laiyemo, Emmanuel Fadiran, Monica Yu, Beverly Gallauresi, Ameeta Parekh Office of Women’s Health, FDA, 10903 New Hampshire Ave. Silver Spring, MD 20993. INTRODUCTION.

E N D
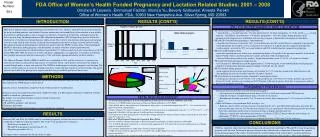
Poster Number: B13 FDA Office of Women’s Health Funded Pregnancy and Lactation Related Studies: 2001 – 2008 Omolara R Laiyemo, Emmanuel Fadiran, Monica Yu, Beverly Gallauresi, Ameeta Parekh Office of Women’s Health, FDA, 10903 New Hampshire Ave. Silver Spring, MD 20993 INTRODUCTION RESULTS (CONT’D) RESULTS(CONT’D) PK / PD IN PREGNANCY AND LACTATION More than 4 million women in the United States give birth every year. Of these, about 64% are given prescriptions for drugs excluding minerals and vitamins. Pregnant women may need prophylaxis for bioterrorism or may need to be treated for underlying illness such as urinary tract infection, respiratory tract infection, and hypertension. Yet, little is known about the pharmacokinetics (PK) and pharmacodynamics (PD) of many drugs that are used in the treatment of several diseases during pregnancy and lactation. This is due to non-inclusion of pregnant and lactating women in many clinical trials because of concern for teratogenicity and safety of drugs secreted into breast milk. Physiological changes during pregnancy and lactation greatly affect the PK/PD of many drugs. Understanding the PK/PD of these drugs during pregnancy and postpartum are unmet needs that require urgent attention. The CDC’s National Center for Health Statistics reported that 10.7 million women used oral contraceptives in the US during 2006-2008. With the rising use of herbs and dietary supplements, it is imperative to recognize and identify their possible interactions with oral contraceptives. This will enable appropriate labeling for these products. The Office of Women's Health (OWH) at the FDA was established in 1994 with the mission to: 1) advocate for inclusion of women in clinical trials and analysis of sex/gender effects, and 2) protect and advance the health of women through policy, science, and outreach. The OWH has funded projects related to pregnancy and lactation. The objective of this study was to assess the findings from these studies and their impact on women’s health. This poster presents the results of the principal investigators and does not present FDA position on these issues. • PK of amoxicillin during pregnancy and postpartum • amoxillin CLrenal (second trimester - 24.8 L/h, third trimester -24.0 L/h, postpartum -15.3 L/h) and CLsecretion (second trimester - 280 ml/min , third trimester - 259 ml/min, postpartum – 167) were higher during pregnancy than postpartum reflecting increases in filtration and secretory transport or diminished reabsorption in the kidneys. • PK and PD of atenolol during pregnancy and postpartum • atenolol renal clearance increased by 38% in second trimester and 36% in third trimester compared to postpartum. • atenolol half-life decreased by 12% in second trimester and by 11% in third trimester compared to postpartum. • cardiac output increased by 20% in second trimester and 28% in third trimester compared to postpartum • PK of atenolol during lactation • atenolol concentrations were below assay quantification limits (<10 ng/mL) in the plasma of normal 3-4 month old infants. Further study is needed in premature infants and infants with renal impairment. • Atenolol infant doses relative to the mother’s weight-adjusted doses were 5.9-14.6% at 2 weeks to 8 months. • PK of labetalol during pregnancy and postpartum • oral clearance of labetalol increased by approximately 1.5 fold during the second and third trimester of pregnancy compared to postpartum, but plasma protein binding of labetalol was not altered • PK of sertraline during pregnancy • mean apparent increase in the oral clearance of sertraline by 15.7% from the second to the third trimester with corresponding decreases in sertraline exposure (except in 1 patient) • PK of azithromycin in pregnant women compared to non pregnant women • azithromycin clearance was 21% lower at 12 weeks gestation age, 25% lower at 24 weeks gestation age and 32% lower at 40 weeks gestation age resulting in 20-30% higher azithromycin plasma levels due to a pregnancy-induced decrease in the biliary excretion. Number of studies METHODS • The final reports or publications of pregnancy and lactation related funded studies between 2001 and 2008 were retrieved from the OWH database and reviewed. • Inclusion criteria: Satisfactorily completed studies with final reports or publications • Exclusion criteria: Incomplete/unsatisfactorily completed studies (e.g. PI resigned, terminated, withdrawal of funds, inability to enroll any participant etc.). • The reports were classified into three categories based on their focus: • Fetal risk assessment, • PK and PD in pregnancy and lactation • Pregnancy prevention • The impact of the results of the studies on women’s health was evaluated. PREGNANCY PREVENTION • Interaction between St John’s wort and an oral contraceptive. • Oral clearance of norethindrone increased from 8.2 L/h to 9.5 L/h, due to increased CYP3A activity • Half-life of ethinyl estradiol reduced from 23.4 hours to 12.2 hours) • Breakthrough bleeding occurred in 2 of 12 women in control phase compared to 7 of 12 women in St John’s wort phase. • Effect of Echinacea on cytochrome P450 activity in vivo • Echinacea increased the systemic clearance of midazolam by 34%, and reduced the midazolam area under the concentration-time curve by 23% but the oral clearance was not significantly altered indicating that the interaction observed is dependent on the relative extraction of drugs at hepatic and intestinal sites • Echinacea significantly reduced the oral clearance of caffeine (CYP1A2) but no effect on oral clearance of tolbutamide (CYP2C9) or dextromethorphan (CYP2D6) • Caution should be used when Echinacea is coadministered with CYP3A and CYP1A substrates. FETAL RISK ASSESSMENT • Use of Automated Databases to Assess Fetal Effects of Maternal Use of Selected Antibiotics and ACEI • Review of >170,000 mother/infant pairs in Tennessee Medicaid database (1985-2000) • Rate of birth defects for ciprofloxacin, azithromycin, doxycycline, or amoxicillin ranged from 2.97% - 3.5% consistent with major birth defects in population • Infants with only first trimester exposure to ACEI had an increased risk of malformation (risk ratio = 2.71; 95% CI 1.72 – 4.27), compared with infants with no exposure to antihypertensive medications • Fetal exposure to other antihypertensive medications during only the first trimester did not confer an increased risk (risk ratio, 0.66; 95 % CI 0.25 to 1.75). • Risk of ACEI in Pregnant Women for Congenital Heart Defect • Review of 465,816 mother/infant pairs in Kaiser Permanente of Northern California database (1995-2008) • Use of ACEIs during first trimester was associated with approximately 29% increased risk of any malformations in offspring compare to normal controls • Use of other antihypertensive medications showed a similar magnitude • ACEI use in first trimester appeared to be associated with a slightly higher risk of any malformation among women with preexisting diabetes • Study did not confirm the of previous finding from Tennessee Medicaid database. RESULTS • Between 2001 and 2008, the OWH funded 9 extramural pregnancy and lactation related studies which were conducted in 7 different centers/institutions. The studies were grouped into 3 categories: • Fetal risk assessment (N = 2) • PK and PD in pregnancy and lactation (N = 6), • Pregnancy prevention (N = 1). • The figures below summarize the details of these studies. CONCLUSIONS OWH has supported studies that had clinical impact and advanced our knowledge of PK and PD of some drugs during pregnancy and lactation. Inclusion of pregnant women in drug clinical trials is imperative to determine the optimal dosing during pregnancy The studies also promoted the understanding of oral contraceptives and herb interactions while demonstrating that recruitment and retention of pregnant women for clinical trials is still a major challenge.