Download
1 / 34
920 likes | 2.82k Vues
Hemolytic disease of newborn. Objectives. Definition & characteristics ABO vs Rh hemolytic disease of the newborn Pathogenesis Incidence Blood types of mother and baby Severity of disease Laboratory data Prevention Rh immune globulin Tests for feto-maternal hemorrhage

E N D
Objectives • Definition & characteristics • ABO vs Rh hemolytic disease of the newborn • Pathogenesis • Incidence • Blood types of mother and baby • Severity of disease • Laboratory data • Prevention • Rh immune globulin • Tests for feto-maternal hemorrhage • Exchange transfusion protocol
Hemolytic disease of newborn Hemolytic disease of the new born and fetus (HDN) is a destruction of the red blood cells (RBCs) of the fetus and neonate by antibodies produced by the mother It is a condition in which the life span of the fetal/neonatal red cells is shortened due to maternal allo-antibodies against red cell antigens acquired from the father
Antibodies • Five classes of antibodies • IgM • IgG • IgA • IgD • IgE • Blood groups specific antibodies are • IgG and • IgM
Biochemistry of antibodies • Made from four polypeptide chains • Two light (L) chains • Two identical heavy (H) chains • Each class has immunologically distinct heavy chain
Blood group antibodies • Blood group antibodies can be classified as • Naturally occurring and immune antibodies • Depending on presensitization • Cold and warm antibodies • Thermal range of antibodies • Most natural Abs are cold & some e.g wide thermal range like Anti A and Anti B • Most immune Abs are warm and can destroy red cell in-vivo • Complete and incomplete antibodies • Depends on agglutination of saline suspended red cells • IgM is complete antibody; most naturally occurring antibodies are complete and of IgM class • IgG is incomplete antibody
Antibodies of ABO system • Anti- A • Naturally occurring • Immune • Anti- B • Naturally occurring • Immune • Anti- A1 • Anti- H
Antibodies of Rh system • Naturally occurring • Anti- E • Occasionally anti-D and anti C • Immune antibodies • D antibodies are more immunogenic • Other are anti c, E, e, C. • Most common is anti- E • After anti- D, anti- c is the common cause of HDN (The vast majority of Rh antibodies are IgG and do not fix complement)
Antibodies from other blood group systems • Anti- K • Kell blood group system • Usually is immune antibody • Warm Ab • Anti- Jka • Kidd blood group system • Usually is immune antibody • Warm Ab
Complement • Complements are series of proteins, present in plasma as an inactive precursors • When activated and react sequentially with each other they mediate destruction of cells and bacteria • Complement activation involves two stages • Opsonization • Lytic stage
Complement • Antibodies can fix complement and cause rapid destruction of red cells • Destruction depends on the amount of antibody and complement • In ABO- incompatible transfusion no surviving A or B red cells can be seen after 1 hour of transfusion • Why? • Remember naturally occurring Abs. are IgM and fix complement mediating the hemolysis
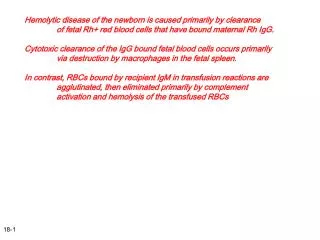
Disease mechanism - HDN • There is destruction of the RBCs of the fetus by antibodies produced by mother • If the fetal red cells contains the corresponding antigen, then binding of antibody will occur to red cells • Coated RBCs are removed by mononuclear phagocytic system
Neonatal liver is immature and unable to handle bilirubin Unconjugated bilirubin Conjugated bilirubin Coated red blood cell are hemolysed in spleen
Pathogenesis; before birth
Pathogenesis; after delivery
Clinical features • Less severe form • Mild anemia • Severe forms • Icterus gravis neonatorum (Kernicterus) • Intrauterine death • Hydrops fetalis • Oedematous, ascites, bulky swollen & friable placenta • Pathophysiology • Extravascular hemolysis with extramedullary erythropoiesis • Hepatic and cardiac failure
Hemolytic disease of newborn HDN BOFORE BIRTH • Anemia (destruction of red cells) • Heart failure • Fetal death AFTER BIRTH • Anemia (destruction of red cells) • Heart failure • Build up of bilirubin • Kernicterus • Severe growth retardation
P N Blood film of a fetus affected by HDN showing polychromasia and increased number of normaoblasts
Rh HEMOLYTIC DISEASE OF NEWBORN • Antibodies against • Anti-D and less commonly anti-c, anti-E • Mother is the case of anti-D is Rh -ve (negative) • Firstborn infant is usually unaffected • Sensitization of mother occurs • During gestation • At the time of birth • All subsequent offspring inheriting D-antigen will be affected in case of anti-D HDN
Pathogenesis Fetomaternal Hemorrhage Maternal Antibodies formed against Paternally derived antigens During subsequent pregnancy, placental passage of maternal IgG antibodies Maternal antibody attaches to fetal red blood cells Fetal red blood cell hemolysis
Diagnosis and Management • Cooperation between • Pregnant patient • Obstetrician • Her spouse • Clinical laboratory
Recommended obstetric practice • History; including H/O previous pregnancies or and disease needing blood transfusion • ABO and Rh testing • Antibody detection; • To detect clinically significant IgG Ab which reacts at 370C • Repeat testing required at 24 or 28 weeks if first test negative • Antibody specificity • Parental phenotype • Amniocyte testing
Antibody titres • Difference of 2 dilutions or score more than 10 is significant • Amniocentesis and cordocentesis • Concentration of bilirubin • Spectrophotometric scan • Indirect method • Increasing or un-change OD as pregnancy advance shows worsening of the fetal hemolytic disease • Fetal blood sample can be taken and tested for • Hb, HCT, blood type and DCT (Direct Coombs test) Percutaneous Umbilical blood sampling
Prevention of Rh- HDN • Prevention of active immunization • Administration of corresponding RBC antibody (e.g anti-D) • Use of high-titered Rh-Ig (Rhogam) • Calculation of the dose • Kleihauer test for fetal Hb
Mechanism of action • Administered antibodies will bind the fetal Rh- positive cells • Spleen captured these cells by Fc-receptors • Spleen remove anti-D coated red cells prior to contact with antigen presenting cells “antigen deviation”
The Kleihauer test • The identification of cells containing haemoglobin F depends on the fact that they resist acid elution to a greater extent than do normal cells, they appear as isolated, darkly stained cells among a background of palely staining ghost cells. • The occasional cells that stain to an intermediate degree are less easy to evaluate; some may be reticulocytes because these also resist acid elution to some extent.
ABO HEMOLYTIC DISEASE OF NEW BORN • For practical purpose, only group O individuals make high titres IgG • Anti-A and anti-B are predominantly IgM • ABO antibodies are present in the sera of all individuals whose RBCs lack the corresponding antigens
ABO HDN contd. • Signs and symptoms • Two mechanism protects the fetus against anti-A and anti-B • Relative weak A and B antigens o fetal red cells • Widespread distribution of A & B antigen in fetal tissue diverting antibodies away from fetal RBCs • Anemia is most of the time mild • ABO- HDN may be seen in the first pregnancy • Laboratory findings • Differ from Rh- HDN; microspherocytes are characteristic of ABO- HDN • Bilirubin peak is later; 1- 3 days after birth • Collection of cord blood and testing eluates form red cells will reveal anti-A or anti-B • Treatment • Group O donor blood for exchange transfusion which is rarely required
HDN- due to other antibodies • Anti-c • Usually less severe than that cause by Anti-D • Anti-K • May cause severe fetal anemia • Blood transfusion for the treatment should lack the appropriate antigen
Summary. • Hemolytic disease of newborn occurs when IgG antibodies produced by the mother against the corresponding antigen which is absent in her, crosses the placenta and destroy the red blood cells of the fetus. • Proper early management of Rh- HDN saves lives of a child and future pregnancies • ABO- HDN is usually mild • Other blood group antigens can also cause HDN