GHCCG as an Organisation
140 likes | 313 Vues
GHCCG as an Organisation. Carol McKenna Designate Chief Officer. PCTs and CCGs – the Differences. Membership. CCGs’ most important element – what sets them apart from predecessors Governing Body must remember it acts on behalf of its members Complex accountability arrangements

GHCCG as an Organisation
E N D
Presentation Transcript
GHCCG as an Organisation Carol McKenna Designate Chief Officer
Membership • CCGs’ most important element – what sets them apart from predecessors • Governing Body must remember it acts on behalf of its members • Complex accountability arrangements • Brings huge potential to deliver improvement in quality, outcomes, and use of resources • Accountability, innovation and reward
Greater Huddersfield CCG Our Vision ‘being informed by our local population and clinicians, we will drive improvement of healthcare services through leadership, innovation and excellence’
Our Values • Listening to health professionals, local people and those who support the CCG, in the commissioning of high quality healthcare in the most appropriate setting • Learning from other CCGs, service providers, the local authority and the NHSCB to inform a strategic , long term vision for change • Leading through enthusiasm and cohesiveness to reduce health inequalities in Greater Huddersfield • Enabling local people and clinicians to transform and improve Greater Huddersfield’s health and healthcare
Current Situation • CCGs become statutory, accountable organisations from 1 April 2013. • PCTs end on 31 March 2013 • CCG authorisation process underway – we are wave 2 • Culminates in site visit on 19 October • Final decision in December
Our Governance arrangements Changes between now and April 13 NHS CKW Cluster CCG Governing Body Clinical Commissioning Executive Audit & Governance Quality Finance & Performance Remuneration Committee Senior Management Team/Clinical Strategy Group/Organisational Development (Operational Groups)
Why does governance matter? • Gives clarity on decision making • Brings a range of perspectives to help make the right decision • Provides confidence and assurance to others eg practices and the population • Makes it easier to manage conflicts of interest
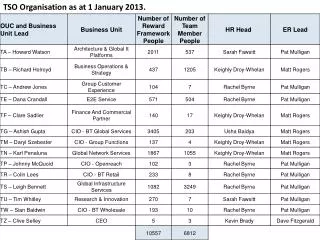
Chief Officer Carol McKenna Clinical Chair Steve Ollerton Greater Huddersfield CCG Structure Chief Financial Officer (Shared) Julie Lawreniuk Head of Contracting & Commercial Strategy 8C Head of Strategic Planning & Service Redesign 8C Governance and Corporate Manager 8A Head of Practice Support & Development 8C Head of Quality & Safety (Shared) 8C Head of Finance (Shared) 8C Shared Financial Services:1/3 of cost shared across 3 CCGs 1.5 x Band 8a; 1 x Band 6; 1 X 4, 0.5 x Band 3 CCG/LA Joint Commissioning Team* Shared Contracts Team 2 x 8a, 1 x 7, 1 x 5 1 x 4 Project Support 3x 5, 1 x 4 Medicines Management Manager* 8C CCG Finance team 1 x 8a, 2 x 7, 1 x 5 Performance Manager 7 Safeguarding Team Across 3 CCGs 3 x 8b. 1 X 7, 1 x4 Senior Admin - 1 x 5 Admin Officers – 3 x 3, 1 x 2 Practice Support Officers 2 x 6 Programme Management & Delivery 2 x 8a, 1 x 7 Quality Manager 8A Project Support 1 x 5 Continuing Care Team* Practice Pharmacists 1.5 x 8a, 1.5 x 7 Technicians 0.35 x 6, 2 x 5 Green boxes within the structure represent teams or posts which will be shared with other CCGs
Financial Model – Running Costs £m Clinical Costs Management Team CSU Costs Other Costs Contingency Running Cost Allowance 0.9 1.6 2.0 0.7 0.5 5.7
Listening to health professionals, local people and those who support the CCG, in the commissioning of high quality healthcare in the most appropriate setting Learning from other CCGs, service providers, the local authority and the NHSCB to inform a strategic , long term vision for change Leading through enthusiasm and cohesiveness to reduce health inequalities in Greater Huddersfield Enabling local people and clinicians to transform and improve Greater Huddersfield’s health and healthcare Strategic Planning (ie, what, why, when and how) • GHCCG Operational Plan 2012/13 produced in February 2012 • Still in the final year of the PCT strategic plan • Now considering our own medium – longer term plans • Cannot do this purely on our own – HWBB and strategic review are important • QIPP is integral to planning
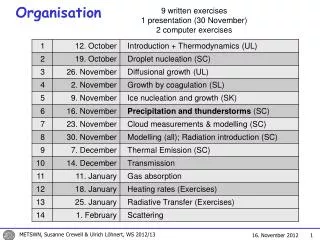
Timeline for 13/14 planning End Nov Prioritised to support alignment of resources/ capacity/capability Dec with CCG practices; staff; Stakeholders August OD workshop By End OCT recommend framework/ reporting templates. Update GHCCG QIPP reporting framework Start Aug Align SR/ CCG practices options Agree themes Novframe the priorities/ objectives