Download
1 / 22
220 likes | 267 Vues
This programme addresses the growing needs of East Lancashire's population, focusing on chronic diseases such as CVD, COPD, diabetes, and dementia. By providing proactive care in the community, the initiative aims to reduce hospitalization and improve outcomes for individuals with long-term conditions. Through risk profiling, integrated care teams, and shared decision-making, the programme strives to empower patients and deliver quality care closer to home. Strategic collaborations with local authorities and partners ensure seamless pathways of care and cost-effective solutions.

E N D
Intermediate Care Programme and Telehealth East Lancashire Susan Warburton MSc, RGN Head of Community Services
Key Facts • East Lancashire population 376,000 • Diverse - geography/urban/rural - population/ethnic - prosperity/poverty • By 2015 > 65 years increase by 17.3% in East Lancashire • Incidence rate dementia increasing • Prevalence of chronic diseases > 65 years increasing • High impact areas • CVD • COPD • Diabetes • Dementia • LCC spend £13 million on intermediate care related services • NHS East Lancashire spend £26.4 million • Outcomes of that spend poor/multiple duplication of service • 70% of existing health and social care costs are used on people with LTC • 60% increase in the number of people with more than one long-term condition within the next decade • Savings required of £56 million over 3 years to balance the books • Every GP and health and social care practitioner knows that most of their time is spent caring for people with long-term conditions Ignoring the problem is not an option!
Strategic Direction • Supporting People with LTC’s (DH 2005)highlighted the need to provide proactive care in the community to keep people managing their LTC’s • Our Health, Our Care, Our Say (DH 2006) • Meeting Patients Needs programme committed to provide Care Closer to Home (2007) – LTC care stream redesigning pathways • Putting People First (DH 2007) • Commissioning Strategic Plan 2008 has intermediate care in the community as a high level priority • Transitional Care Project commissioned in 2009 joint endeavour with LCC/ELPCT • Significant evidence base that care closer to home provides quality of outcome at reduced cost • Transforming Community Services (2010) • Operating Framework 2011 • Vision for Adult Social Care (DH 2010) • Intermediate Care-Half way Home (DH 2009) • Ready to Go (DH 2010) • Intermediate care programme reflects the commissioning intentions of GP commissioners to commission integrated community services that support care closer to home or when possible in the home • Integrated working with LCC and other partners to achieve the seamless pathways of care together with the inherent cost benefit • Case management model - TCS
Evidence Integrated working between health, social care and partners reduce bed usage and emergency admissions (Torbay) SPA-good communications-integrated records, involvement of VCFS (Third Age) prevent readmissions and improve outcomes for older people (Cumbria) Independent sector can bring innovation, investment and transformation in integrated service provision (Serco) Virtual wards – hospital avoidance (Wandsworth) Same day access to primary care, easy access to specialist, the use of IT and access to test results reduce demand and improve outcomes (Brent)
What Patients Tell Us! • They want to be supported and their care needs managed in their own home or as close to their homes/community as possible • They are concerned that community services will not be able to provide enough support to enable them to be properly supported to self manage their condition • As their condition evolves they are concerned about their options and feel that hospital is a safe place hence increasing hospitalisation of ASC • Social isolation is mentioned by older people and for those who are disabled by long term conditions as a concern – fear of staying at home
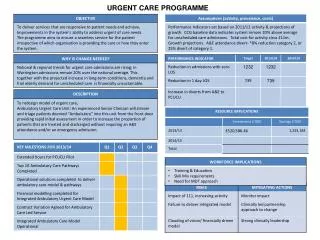
LTC QIPP • Improving outcomes for those with a LTC by delivering local, efficient, patient focused services • Responsive management of conditions that reduce the need for costly hospitalisation
LTC QIPP • RISK PROFILING - Using risk profiling to ensure that teams understand the needs of their population and manage those at risk. Will allow for interventions to be targeted and prioritised. • INTEGRATED CARE TEAMS - The creation of integrated health and social care teams based around a locality (or neighbourhood). These generic teams pull in specialist services when necessary, but treat a patient holistically instead of the condition. Joined up, productive care • SELF CARE / SHARED DECISION MAKING – Seeing patients as experts in their condition and empowering them to seek the information, care and support they need when they need it. ‘No decision about me without me’ • All have to be in place to get results!
IMPROVED QUALITY INTEGRATION CHOICE WORKFORCE DEVELOPMENT PERSONALISATION PATIENT CLINICAL LEADERSHIP CARE CLOSER TO HOME IMPROVED OUTCOMES & EXPERIENCE SAFER SERVICES Generic Workforce Health and Social Care - Robust ClinicalLeadership - Multi-DisciplinaryTeams - Greater use of technology - Shared information systems - Developing community services 24/7 365 days - Joint education and training including the 3rd Sector Demand Management Managing patient flows back to community (i.e. referring patients back to the community sooner)Preventing Admissions and readmissions East Lancashire’s Intermediate Care Vision Patient Centred Care Single AssessmentsOutcome based assessments Personal Care PlansSelf Management (LTC)Personal Health/Social Care BudgetsPersonal Sanctuary (EOL)Long term Care Coordination Improved CommunicationPatient & Public InvolvementSocial Marketing Working with 3rd Sector Pathway Redesign AreasUrgent care – timely and effective dischargeUrgent care – admission avoidanceLong term conditions (including Mental Health)End of LifePlanned Care Measurable OutcomesReduced numbers of admissionsReduced lengths of staysImproved Patient OutcomesImproved Patient and Service ExperienceDifferent Financial Models
Rehabilitation and Reablement Funding • Additional funding from the DH to support rehabilitation/reablement • Notification that from 2012 acute providers will be responsible for care 30 days post discharge • Requirement to work in a collaborative manner with LCC and providers to ensure integration of pathways for service users, innovation in deliver of care and development of responsive services
Progress to date • Joint business case produced with LCC –vision for future integration • Event November 2010 – GP Commissioners Shaping the Future • Commissioning intentions stated 11/12 contract notice given (rehab) • Governance structures in place with partners • Work streams established at East Lancs level – joint project management • Redesign of integrated therapy with reablement being undertaken
Continued • Redesign of community nursing service • Virtual ward pilot programme in Pendle in collaboration with LCC-now rolling out across East Lancashire • Cost benefit analysis/business case being worked up • LCC redesigned residential rehabilitation to include night time support and extra health support e.g. GP assessment
Continued • Joint Commissioning Strategy for Dementia produced • Integrated strategy for End of Life care developed by EOL project group • LCC Crisis support services re-modelled to provide consistent service delivery across EL • Tested the use of independent sector intermediate care beds • ICAT commissioned • EMIS web roll out will be completed by March 2013 • Telemedicine/telehealth project to commence
Continued • Needs assessment of patients undertaken in community hospitals triangulated with other data • Review of extra care accommodation and intermediate care support available • Beginning to review and look at options for new models for intermediate care in the community i.e. different housing models – Belong • Business case being drawn up around the support of those with dementia (LTC) in the community
Virtual Ward • Pilot programme – 12 months Dec 2010 • Whole system approach needed to shift care delivery- working with partners • 3 levels • Promotion of self care and condition management e.g. COPD care bundle • Encouragement to live more independently at home • Redesign in the way community services are delivered
What did we do? • Pilot in Pendle • Invested in community equipment response • Invested in social workers • Invested in therapy locum support • Invested time in communication with practices/LCC provider • Community nursing staff redesign to change focus – more responsive • Daily ward rounds - teleconference
Evaluation • Provider staffing costs • Details of GP/OOH call out • Prescribing costs/medicines management • Use of equipment • Cost of diagnostics • Therapy input • Detailed activity assumptions and case mix • Costs across the pathway into social care • Patient experience
Telehealth Project • Project being developed in collaboration with InTechnology- 2 year pilot • Project began in May 2012 and will begin to recruit patients in September 2012 • Focus will be initially on the COPD pathway to trial the project – 200 patients per year • Dedicated project manager
The Project • Consultancy support • Training and Education of staff • Web enabled portal for staff and patients-self management support • Completely managed service supported by NHS Direct • Development of pathways • 7 days per week • Linked to virtual ward-side ward • Patients risk profiled to identify appropriate patients – level 2-3 patients
Outcome • Allow the individual to develop the knowledge and skills to manage condition • Allow health professionals to target their efforts where required • Improve patient experience of health care/increase confidence • Reduce health inequity by providing a different approach • Reduce hospitalisation by proactive interventions • Slowing disease progression due to proactive connected management
Next Steps Continue to work with partners to build on the strong foundations that we have put down over the past 2 years Work with LCC and partners in the alignment of telecare to current intermediate care projects Further develop the preventative and self management community infrastructure e.g. hand rails, slipper exchange Further develop collaborations with housing associations and others to promote improvement in housing stock that will meet the needs of the aging population thus supporting care closer to home vision Continued partnership working with VCFS and other partners e.g. hospital aftercare service (Age UK)
THANK YOU ! Susan Warburton Head of Community Services East Lancashire PCT Tel:01282 644881 Email: susan.warburton@eastlancspct.nhs.uk