Download
1 / 42
460 likes | 724 Vues
Explore latent, tertiary, and congenital syphilis phases, diagnosis methods, and treatment options. Learn about gummas, neurosyphilis, and cardiovascular syphilis manifestations. Understand the impact on pregnancy and newborns.

E N D
Tertiary and congenital syphilis. Principles of therapy and prophylaxis. Lector: Shkilna M.
"He who knows syphilis, knows medicine" Sir William Osler
Content 1. LATENT SYPHILIS 2. TERTIARY SYPHILS 3. CONGENITAL SYPHILIS • Early congenital syphilis; • Late congenital syphilis 4. Treatment 5. Treatment in Pregnancy 6. Jarisch-Herxheimer reaction
LATENT SYPHILIS The period between secondary and tertiary syphilis. Early latency: the first 4years when secondary relapses may occur. Late latency is the asymptomatic period beyond 4 years. During this latter period, the patient harbors infectious organisms, especially in the spleen and lymph nodes and blood serology remains positive.
World War II Poster: Both of These Men Had Syphilis 1/3 of untreated pts will proceed to tertiary syphilis
TERTIARY SYPHILS is a no contagious but highly destructive phase of syphilis which may take many years to develop; it may manifest itself in several forms: Gummas Neuro-syphilis Cardiovascular Syphilis
Gummas It develops in 15% of untreated cases within 1-10 years after infection. highly destructive tertiary syphilitic lesions that usually occur in skin and bones but may also occur in other tissues. Slowly progressive, painless, dull red nodule or plaque. Breakdown into ulcer with wash-leather floor. Regional Ln are not enlarged. Not infectious.
Cardiovascular Syphilis • 10% of untreated syphilis cases develop CDS 10-40 years after initial infection. • Heart: CDS occurs due to localized affection (gumma) or generalized affection that leads to heart failure. • Aorta: aortic regurge, aneurysm or coronary osteal stenosis.
Neurosyphils Asymptomatic Symptomatic
Asymptomatic neurosyphilis in which there are no symptoms of CNS involvement but the CSF is abnormal: Elevated lymphocytes Elevated protein. Positive CSF VDRL tests Approximately 20% of these patients progress to symptomatic neurosyphilis
Symptomatic Neurosyphilis Symptoms of neurosyphilis: 8% of untreated cases. 5-35 years after infection. Invasion of the CNS occurs early when generalized dissemination occurs (2° syphilis).
Diagnosis of congenital syphilis • Mothers anamnesis • Examination of placenta and umbilical cord • Assessment of typical characteristics of congenital syphilis in different growing group • Treponema pallidum can be demonstrated in a smear from skin lesions with moist surface. • Assessment of eye ground • An X-ray examination of the long bones • Clinical assessment of parents.
Possible results of pregnancy, according to the time of affection of pregnant: • Abortion ( pregnant affected by syphilis before pregnancy or during first month of pregnancy) • Stillbirth ( pregnant affected by syphilis during 4 -5 month of pregnancy) • Birth of child with congenital syphilis ( pregnant affected by syphilis during 6 -7 month of pregnancy) • If pregnant affected by syphilis during last 1,5-2 month of pregnancy, fetus can affected from mother in delivery during passing through an infected canal
CONGENITAL SYPHILIS Early congenital syphilis: • occur before the age of 1 year; • occur in children from 1 to 4 year. • a) late syphilitic ophtalmopathy (involvement of the eyes); Late congenital syphilis: • b) other forms of the late congenital syphilis (involvement of the skin, mucous membrane, nervous system, latent syphilis).
Syphilis of placenta • Placentais edematous, pale, greasy and bulky. • Weight of placentais 800-900 g (500g in normal). • Placentais more than one-fourth of fetal body weight ( more than one- fifth in normal). • Treponema pallidum can be demonstrated in a smear from placenta ( that’s why it is very contagious).
Syphilis of fetus • Maceration of fetus. • Sometimes dead. • Little weight. • Enlargement of liver and spleen. • Lungs are enlarged, thick, grey-yellow in their color (“Pneumonia Alba”).
Congenital syphilis:of children before the age of 1 year • Syphilitic pemphigus • Diffuse infiltration • Syphilitic rhinitis • Osteochondritis • Syphilitic chorioretinitis
Syphilitic pemphigus • Present after burning or appeared within the first days ore weeks of life. • Consists of bullas 0,5-1 sm.in dm. • Vesicles and erosions distributed bilaterally and symmetrically on the front of the palms and soles. • Treponema pallidum can be demonstrated in a smear from bulla.
Diffuse infiltration • Appeared within the first weeks or month of birth around angles of mouth, lips, buttocks, palms, soles and anus. • Zones of affection are flat ,thick ,yellow-brawn in color with shinny surface. • Later fissuring of lips, deep fissures at the angles of the mouth may be seen, after recovering of which we can see specific fusiform radial atrophic scars.
Syphilitic rhinitis • Nasal breathing is difficult. • Highly infectious purulent-serous and hemorrhagic nasal discharges ( snuffles). • Breathing is hoarse and by mouth. • Nasal septum is dislocated or destroyed with the future deformation of the nose.
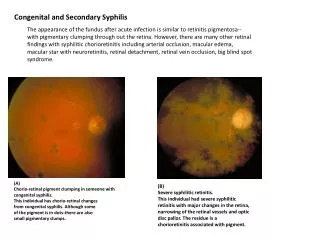
Syphilitic chorioretinitis Assessment of eye ground show points of pigment and zones of depigmentations - symptom of “salt- and-pepper”
Osteochondritis • The main specific and characteristic changes of the bones in patient with congenital syphilis in children before the age of 1 year • Appeared in intrauterine period and cant be diagnose till the end of 1 year of birth • During X-ray examination we can see light strips 0,5-1,5 mm ( breach of ossification cartilage) between metaphysic and epiphysis • On josses places bones fractures can appear
Congenital syphilis Papulosquamous Plaques
Congenital syphilis – snuffles and rash
Rhinitis (snuffles), mucous patches, damage to palate (late) Bullae and vesicular rash on soles Eroded papular lesions
Broken vesicles, desquamation Condylomata around anus Infiltration, desquamation and rhinitis
Congenital syphilis:of children from1 to 4 year • Condiloma lata can also appeared on genital organs, inguinal folds, perianal zones with moister surface and large amount of Treponema pallidum . • Pustules, nodules, erosions of mucous membranes of oral cavity. • Affection of bones, inner organs and nerves system can be present. • Certain amount of papules in extremities, buttocks, genital organs, on the inguinal folds. They can be moister. Erosions with a large amount of Treponema pallidum on their surface.
Late congenital syphilis Can appear in 5-20 years old and later is characterized by many specific changes in the: • Skin • Bones • Mucous membranes • Inner organs • Nerve system • Sensitive organs
International classification of late congenital syphilis • Late syphilitic ophtalmopathic (involvement of the eyes). • Late congenital neurosyphilis. • Others form of late congenital syphilis • Affection of bones • Affection of teeth (Hutchinson’s teeth) • Hutchinson’s triad ( interstitial keratitis, Hutchinson’s teeth, eight nerve deafness).
Hutchinson's teeth • Characteristic notched edges • "screwdriver" shaped central incisors
Primary, Secondary, Early LatentSyphilis Recommended regimen -Benzathine Penicillin G, 2.4 million units IM Penicillin Allergy* -Doxycycline 100 mg twice daily x 14 days or -Ceftriaxone 1 gm IM/IV daily x 8-10 days (limited studies) or -Azithromycin 2 gm single oral dose (preliminary data)
SyphilisLatent Syphilis Recommended regimen Benzathine penicillin G 2.4 million units IM at one week intervals x 3 doses Penicillin allergy* Doxycycline 100 mg orally twice daily x 28 days or Tetracycline 500 mg orally four times daily x 28d
Latent SyphilisResponse to Treatment • Limited data available to guide evaluation • Repeat RPR(VDRL) at 6, 12, 24 months • Perform CSF exam & re-treat for latent syphilis, if: • 4x increase in titer, • initial nontreponemal titer >1:32 fails to decline 12-24 mo after tx, or • signs/sx
Jarisch-Herxheimer reaction Manifestations: general malaise, fever, headache, sweating, rigors, or a temporary exacerbation of the syphilitic lesions. Usually seen w early syphilis, especially secondary syphilis. Seen within 6 to 12 h of initial treatment. Usually subsides within 24 h and poses no danger but may produce anxiety. However, patients with general paresis or a high CSF cell count are likely to develop serious disorders, such as seizures or strokes. It may be confused with allergy to antibiotics. May indicate coexistent syphilis in patients treated for other conditions with antibiotics active against syphilis This reaction should be explained to the patient before treatment.