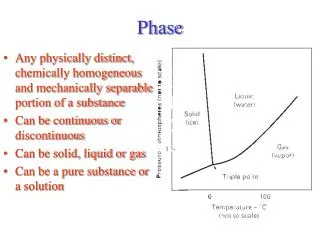
Maintenance Phase
250 likes | 421 Vues
Maintenance Phase. Judith Martin, MD Medical Director, The 14 th Street Clinic, Oakland. Clinical tasks of maintenance phase:. Stable medication as a platform Monitoring progress in treatment Managing threats to stability Referrals for higher level of care. rapport. engagement.

Maintenance Phase
E N D
Presentation Transcript
Maintenance Phase Judith Martin, MD Medical Director, The 14th Street Clinic, Oakland
Clinical tasks of maintenance phase: • Stable medication as a platform • Monitoring progress in treatment • Managing threats to stability • Referrals for higher level of care
rapport engagement support attendance RETENTION IN TREATMENT stability stability stability
Groundwork • Initial agreement with patient • Initial questionnaires • Initial problem list and assessment • Stabilized dose schedule • Home meeting/counseling
Examples of Patient agreements: • to take the medication only as prescribed • to notify the clinic immediately in case of lost or stolen medication • to comply with the required pill counts and urine tests.
Integrating care:Examples from Patient Intake Questionnaire How do you achieve peace of mind? What are your sources of inner strength? What are your best qualities?
INTEGRATING CARE:PATIENT QUESTIONNAIRE ABOUT RELAPSE • What ‘triggers’ do you know which put you in danger of relapse to drug abuse? • What coping methods have you developed to deal with these triggers to relapse?
Adjustment to chronic disease Grief process Hope for cure or mild case Life changes needed Specifics of addiction: social milieu dangerous supports burned out coping by drug a pattern
Periodic monitoring • Protocol for random testing • Periodic observed dosing • Relapse prevention/ongoing behavior change • Periodic physical examination/labs
MONITORING Urine toxicology screens: On -Site at each visit Send -away initial and yearly Random call twice a year Pill counts at each visit Breathalyzer: initial, then individualized Physical exam: initial, annual and individualized Labs: initial, then individualized, some annual Physical comfort at dose
Monitoring Treatment Progress • Drug use must be a primary measure of treatment progress • How to measure? • Self-report? • Report of spouse or other concerned party? • Drug Testing: urine? sweat? hair? • Changes in drug associated behaviors? Stealing, drug-dealing
Urine Testing • Develop Standard Collection procedures for in office or off site testing • Observed vs. not observed
Reasonable alternative to watching • Urine collection container with temperature strip
Reasonable alternative to watching • Urine collection container with temperature strip
Treatment Outcome Data:Methadone Maintenance • 8-10 fold reduction in death rate • reduction of drug use • reduction of criminal activity • engagement in socially productive roles • reduced spread of HIV
THREATS TO STABILITY • Other drug abuse or positive screens • Medical problems • Life changes: moves, divorce, new job
RED FLAGS CHECKLIST • Missing appointments • Running out of medication too soon • Taking medication off schedule • Not responding to phone calls • Refusing urine or breath testing • Neglecting to mention new medications or outside treatment
RED FLAGS CHECKILST,cont. • Appearing intoxicated or disheveled in person or on the phone • Frequent or urgent inappropriate phone calls • Neglecting to mention change in address, work, or home situation • Inappropriate outbursts of anger • Lost or stolen medication
RED FLAGS CHECKLIST,cont. • Frequent physical injuries or accidents • Non-payment of visit bills
RESPONSE TO RED FLAGS Address with patient as soon as noticed Ask for self-evaluation Ask for patient-generated plan Formalize plan within office limits Written contract may be needed HAS TO MAKE SENSE FOR THIS PATIENT
STAGES OF CHANGE:MAINTENANCE • Solidify gains of the active phase • Work to prevent relapse • Consistently engage in new behavior
RELAPSE -Regress to earlier “stage of change” -Relapse and recycling is the rule, not the exception. -Most relapse is to contemplation. -Some people benefit from recycling.
MONITORING:META-MESSAGES Stability allows progress Progress in treatment is expected and encouraged Relapse does not necessarily mean complete failure It’s important to have people who ‘watch out for you’ Addiction treatment is not just a pill Structure varies depending on progress
MONITORING: SUMMARY Regular follow-up visits Regular and random testing and pill counts Address red flag behavior promptly Adjust structure and contracts according to progress What you are doing should make sense
Referral and discontinuation • Higher level of care needed • Immediate dismissal for behavior • Taper for administrative non-compliance • (clear guidelines important)