Download
1 / 27
300 likes | 351 Vues
Learn about the therapeutic targets, progression, and right ventricular failure in managing cardiogenic shock. Explore goals of care and pathways for establishing effective treatment strategies. Understand the importance of percutaneous circulatory support and available therapies 24/7 in different medical programs.

E N D
Key elements of a cardiogenic shock team Sandeep Nathan, MD, MSc, FACC, FSCAI Associate Professor of Medicine Medical Director, Cardiac Intensive Care Unit Director, Interventional Cardiology Fellowship Program Co-Director, Cardiac Catheterization Laboratory University of Chicago Medicine | Chicago, IL Getingesymposium | SCAI 2019 | Las Vegas
Disclosures Company Affiliation/Financial Relationship • Grant / Research Support None relevant • Consulting / Advisory Panel / Honoraria Abiomed Cardiovascular Systems, Inc Getinge Terumo Interventional Systems • Major Stock Shareholder/Equity None • Royalty Income None • Ownership / Founder None • Intellectual Property Rights None • Other Financial Benefit None 2 ML-0801 Rev A/MCV00091529 REV A
Therapeutic targets in the management of cardiogenic shock 3 ML-0801 Rev A/MCV00091529 REV A
Progression of cardiogenic shock from a hemodynamic problem to a cardiometabolic syndrome Clinical stability ECG ’s, sxs, cardiac biomarkers MAP, LV-ESP & EDP Aortic pulse pressure Pulmonary edema, BNP, Neuro ’s, lactate ECG ’s, biomarkers, ventricular arrhythmias Creatinine, LFTs, lactate, coagulopathy Myocardial ischemia Hemodynamic instability Volume overload & systemic hypoperfusion Coronary perfusion End-organ dysfunction Culprit PCI Vasoactives LV/RV unloading w/pMCS Escalation of pMCS / devices in combo? Complete revasc? Renal & hepatic unloading, renal replacement Rx Death Reyentovich, A., et al. Nature Reviews Cardiology 2016. 4 ML-0801 Rev A/MCV00091529 REV A
Right ventricular failure (RVF) / RV shock • Right ventricular failure (RVF) results from any structural or functional process(es) that decrease the RV’s ability to pump blood into the pulmonary circulation • RVF and/or RV shock are rarely seen in isolation in the critically ill patient outside of pure RV infarction • RVF is increasingly being recognized as a key contributing factor to critical illness across a variety of medical and cardiac illnesses • The addition of RVF to critical illness portends poorer outcomes although the magnitude of this negative impact remains poorly characterized • The pathophysiology of RVF, as with LVF, is complex and varied but remains less studied than LV failure 5 ML-0801 Rev A/MCV00091529 REV A
Is it really as distinct as LV- vs. RV-shock? • Hemodynamically defined RV dysfunction is common in AMI-CS and is largely undetected in the absence of invasive hemodynamic assessment Esposito M., and Kapur, N. F1000Research. 2017. Lala A, et al. J Cardiac Fail 2018;24:148–156. 6 ML-0801 Rev A/MCV00091529 REV A
Goals of care in cardiogenic shock Emergency medical providers & primary service (CCU / CVICU) Early recognition & triage 1 Standardized diagnostic criteria Defined classes & stages 2 3 Multimodality assessment of cardiac and end-organ function • Multidisciplinary Cardiogenic Shock Team: • Interventional Cardiology • Advanced Heart Failure & Transplant • CV Surgery • Cardiac Critical Care 4 Early & continuous multidisciplinary input 5 Clear delineation of the initial careplan & escalation strategy 6 Early revascularization (when appropriate) Appropriate selection & early use of MCS 7 8 Rapid escalation (or de-escalation) of care, as required 9 Primary service provider Involvement of consultants & ancillary service providers 10 Improved survival to discharge and beyond 7 ML-0801 Rev A/MCV00091529 REV A
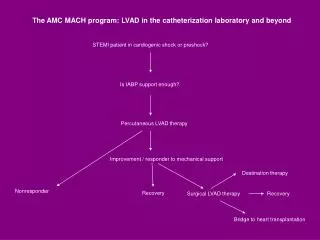
Goals of percutaneous circulatory support • Bridge patients to • Recovery • Decision • Durable VAD • Transplant • Decrease preload • Decrease afterload • Augment cardiac output / power Provide adequate organ perfusion and O2 delivery Support patients through high-risk procedures 8 ML-0801 Rev A/MCV00091529 REV A
Establishing care pathways for cardiogenic shock 9 ML-0801 Rev A/MCV00091529 REV A
What therapies can your center deliver 24/7? • Multiple percutaneous and surgical support devices • VAD and transplant programs • Cardiac arrest & ECLS protocols Quaternary centers / large academic medical centers Level 1 • Percutaneous devices and surgical support options • STEMI program Larger community hospitals Some teaching hospitals Level 2 • No or limited percutaneous support devices Level 3 Smaller community hospitals 10 ML-0801 Rev A/MCV00091529 REV A
Level 1 or “Full-service” program • Primary management: • Advanced heart failure specialist • Interventional cardiologist / Cardiac intensivist • Device deployment / management / escalation: • Interventional cardiologist • Cardiac surgeon • Core team members: • ICU pharmacist • Perfusionist • Advanced cardiac fellows • APN / RN 11 ML-0801 Rev A/MCV00091529 REV A
Level 2 or “Mid-level” program • Primary management: • Heart failure specialist / Interventional cardiologist • (Cardiac) intensivist • Device deployment / management: • Interventional cardiologist • +/- Cardiac surgeon • Core team members: • Pharmacist • Perfusionist • APN/RN 12 ML-0801 Rev A/MCV00091529 REV A
Level 1 care for cardiogenic shock Pathway for instituting a shock program OPERATOR TRAINING, COORDINATION OF CARE DELIVERY, THROUGHPUT & LOGISTICS NURSING, TECH, PERFUSION SUPPORT & ICU CARE INSTITUTIONAL & SPECIALTY-SPECIFIC “BUY-IN” EQUIPMENT & INVENTORY ISSUES SHOCK TEAM APPROACH Clear agreement between all key stakeholders regarding indications, contraindications and programmatic goals. • Key issues: • Hardware ownership, ratios & location • Disposables • Cath lab vs. OR/C-arm vs. procedure room vs. HOR? • ECLS cart Assembly of a 24/7/365 multidisciplinary cardiogenic shock team • Establish initial & repeating training for nurses & techs. • Have a clear understanding with perfusionists. • Train ICU nurses & designate receiving units • Key issues: • Implanting MDs & location, • Explanting MDs, location & timing • Bed geography 13 ML-0801 Rev A/MCV00091529 REV A
Level 1 care for cardiogenic shock Key members of the shock team SUPPORTING STAFF Vascular Surgery Cath Lab: Nurses, Technologists (ideally with 1 “super-user” each) ICU: Nursing leadership support Perfusionists SHOCK TEAM APPROACH Assembly of a 24/7/365 multidisciplinary cardiogenic shock team 14 ML-0801 Rev A/MCV00091529 REV A
Level 1 care for cardiogenic shock Chain of communication within the center 15 ML-0801 Rev A/MCV00091529 REV A
Level 1 care for cardiogenic shock Chain of communication within the center • Key issues to resolve: • Initial care plan including MCS, vasoactive support, ICU care • Identifying NOK / POA • Identifying goals of care / limitations to care • Chart out escalation plan • Decide on timing of next clinical / hemodynamic “snapshot” 16 ML-0801 Rev A/MCV00091529 REV A
Protocolizing cardiogenic shock care ML-0801 Rev A/MCV00091529 REV A
Step 1: Objectively assess, stabilize & perform complete revascularization BEST PRACTICES BEST PRACTICES Activate Cardiac Cath Lab • Access: • Femoral arterial access using micropuncture withimage guidance (ultrasound and/or fluoroscopy)1 • Angiography via 4F micropuncture dilator to confirm puncture site & vessel size • Place appropriately sized (5 or 6 Fr) arterial sheath • Obtain venous access (femoral or internal jugular) Access • Assess Hemodynamics: LVEDP or PAC • If sustained hypotension (SBP < 90 mmHg) for > 30 min • Or • CI < 2.2 with LVEDP or PCWP >15 mmHg,consider mechanical circulatory support Assess Hemodynamics pMCS If femoral arterial anatomy suitable and no contraindications, place, or escalate to(if IABP already in place), Impella 2.5 or Impella CP Begin Weaning Catecholamines* * If consistent with overall hemodynamic management Yes Acute MI? No PCI: Coronary angiography and PCI with goal of complete revascularization. Coronary Angiogramwith PCI • Reassess Hemodynamics: PAC (if not done initially) • CPO = (CO MAP)/451 • PAPi = (sPAP-dPAP)/CVP Reassess Hemodynamics Soverow J, Lee MS. J Invasive Cardiol. 2014;26(12):659-667 CO, cardiac output; CPO, cardiac power output; dPAP, diastolic pulmonary arterial pressure; MAP, mean arterial pressure; PAC, pulmonary arterial catheter; PAPi, pulmonary artery pulsatility index; RA, right arterial pressure; sPAP, systolic pulmonary arterial pressure. 18 ML-0801 Rev A/MCV00091529 REV A
Step 2: Reassessment prior to discharge from cardiac cath lab Reassess Hemodynamics via PAC prior to Discharge from the Cath Lab: • Cardiac Power Output (CPO) = (CO MAP) / 451 • Pulmonary Artery Pulsatility Index (PAPI) = (sPAP-dPAP) / CVP CPO < 0.6 CPO > 0.6 PAPI ≥1 < 1 RV Dysfunction:Right-sided MCS (T/C Impella RP) RV Preserved: Escalate MCS or consider transfer to LVAD/Transplant Center Persistent Hypoxemia? • PaO2 < 55 on 100% FiO2 Consider higher power support device • RV Failure as defined by Recover Right1: • CI < 2.2 L/min/m2 (despite continuous infusion of ≥ 1 high dose inotrope, ie, da/dobutamine≥ 10 µg/kg/min or equivalent) and any of the following: • CVP > 15 mmHg, or • CVP/PCWP or LAP ratio >0.63, or • RV dysfunction on TTE(TAPSE score ≤14 mm) Yes No Admit to ICU to maximizesupportive care and to activelyassess for myocardial recovery Anderson MB, et al. J Heart Lung Transplant. 2015;34(12):1549-1560. 19 ML-0801 Rev A/MCV00091529 REV A
Step 3: Consideration for escalation, weaning and transfer for higher level care Assess for Myocardial Recovery (At least every 12 hours) • Improving • Clinical, Echocardiographic & Hemodynamic parameters (concordant): • ↑ Cardiac output • ↑ CPO • ↑ Urine output • ↓ Lactate • Inotropes low dose/discontinued • Adequate Ramp test • Mixed picture • Clinical, Echocardiographic & Hemodynamic parameters (discordant): • Some parameters are improving • Pressors lowered but not discontinued • Fails “ramp test” • Worsening • Clinical, Echocardiographic & Hemodynamic parameters (concordant): • ↓ Cardiac output • ↓ CPO • ↓ Urine output • ↑ Lactate • Inotrope dependent • Absent pulsatility Myocardial Recovery No Recovery Escalateor Transfer Inadequate Recovery Continue MCS support & frequent clinical reassessment Failure to recover within 48-72 h, consider escalation or durable VAD/transplant Refer to institutional protocol for escalation or transfer Wean & Explant MCS (After a clinically-determined duration of support) 20 ML-0801 Rev A/MCV00091529 REV A
INOVA H&V Institute protocol for CS Compared with 30-day survival of 47% in 2016, 30-day survival in 2017 and 2018 increased to 57.9% and 76.6%, respectively (p < 0.01) Tehrani, B.N. et al. J Am Coll Cardiol. 2019;73(13):1659–69. 21 ML-0801 Rev A/MCV00091529 REV A
INOVA risk prediction model for mortality in CS • Independent predictors of 30-day mortality were age >71 years, diabetes mellitus, dialysis, >36 h of vasopressor use at time of diagnosis, lactate levels >3.0 mg/dl, CPO <0.6 W, and PAPi <1.0 at 24 h after diagnosis and implementation of therapies. • Either 1 or 2 points were assigned to each variable, and a 3-category risk score was determined: 0 to 1 (low), 2 to 4 (moderate), and >5 (high). Tehrani, B.N. et al. J Am Coll Cardiol. 2019;73(13):1659–69. 22 ML-0801 Rev A/MCV00091529 REV A
The Shock Team in action: Clinical profile of a cardiogenic shock patient ML-0801 Rev A/MCV00091529 REV A 24
Profile of an IHCA/CS patient EMS ED IC 57 yo male presenting off-hours w inferior STEMI , sx to door: 60-90 min, hemodynamically stable in ED; door to cath lab transport: 27 min As patient brought to CCL, PMVT VF arrest. 25+ minutes of intermittent cardiac arrest with LUCAS-assisted CPR; IABP considered but Impella CP used 2/2 lack of organized rhythm. PCI performed of large RCA with heavy thrombus burden. ROSC regained after RCA opened; patient transferred to CCU intubated, on low-dose epinephrine gtt and Impella CP with intravascular cooling started but terminated early because of meaningful neurologic activity 1-2 hrs after completion of PCI Patient discharged alive 1 week later with no neurologic deficits & normal LVEF; Alive & well 6+ mo. later, back to working full time IC/CICU IC+HF+ CV Surg IC+HF+ CICU IC/Gen Card ML-0801 Rev A/MCV00091529 REV A
Ideal profile of the IHCA/CS patient * Images used with the patient’s permission. ML-0801 Rev A/MCV00091529 REV A
Summary • Cardiogenic shock represents a dynamic set of conditions, presentation profiles and pathophysiologic mechanisms. Thus, CS care requires continuous monitoring and willingness to adjust the treatment plan. • Biventricular dysfunction is more common than recognized therefore assessment of both RV and LV function is critical. • Time, team and treatment choices are all equally important in combating shock. • Given the lack of clear superiority of any one device, protocols and standardization are keys to success. • Integration of device therapy with system of cares is likely to offer the greatest impact on outcomes. 25 ML-0801 Rev A/MCV00091529 REV A
Thank you! Email: snathan@medicine.bsd.uchicago.edu | Twitter: @SandeepNathanMD 26 ML-0801 Rev A/MCV00091529 REV A