Download
1 / 105
1.05k likes | 1.07k Vues
Explore herbal vs. pharmaceutical approaches for managing joint pain. Understand dosing protocols and test your knowledge on herbal remedies. Learn about traditional NSAIDs, corticosteroids, and natural pain management options without harmful side effects.

E N D
Acute Care Nutrition Workshop John Hess, Ph.D., D.C.N.
Topics to be Covered • Herbal Approach vs. Pharmaceutical • Is there an alternative? • Joint pain • Herbal approaches with a history • Protocols • Understanding dosing • Testing your knowledge • Brief test on herbs covered
Traditional Approach • Non-steroidal anti-inflammatory drugs (NSAID’s) • Corticosteroids • Almekinders, LC. Efficacy of non-steroidal anti-inflammatory drugs in treatment of ligament injuries. Sports Med 1993;9(3):137-42
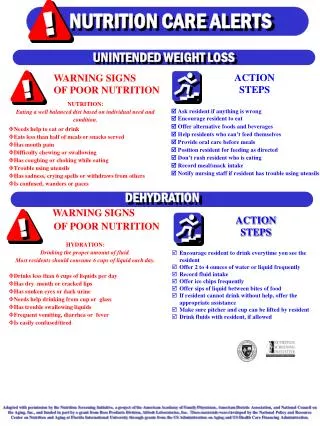
Analgesics For Pain & Inflammation
Fries; Journal of Rheumatology stated • NSAIDs: Are the most widely used class of drugs. • Annually, more than 70 million prescriptions are written, and more than 30 billion NSAIDs are sold OTC in the U.S. • 13 million people in the U.S. use NSAIDs regularly. • The estimated number of annual hospitalizations in the U.S. for serious GI complications is at least 103,000 with direct costs exceeding $2 billion. • There are more deaths annually related to NSAID use than AIDS-related deaths. Fries, JF. NSAID gastropathy: the second most deadly rheumatic disease? Epidemiology and risk appraisal. J Rheumatol 1991; (Suppl 28)18:6-10; Bland J. Nutritional Management of the Underlying Causes of Chronic Disease, Seminar Series. Washington:Institute of Functional Medicine; 2000
Side Effects… • Adverse GI effects of NSAIDs include dyspepsia, occult bleeding, overt bleeding, and “ulcer disease.” • 2 aspirin= 1 tsp of blood lost per day. • Consequences of NSAID-induced GI toxicity include anemia, hospitalization, and death. Garnett WR. GI effects of OTC analgesics: implications for product selection. J Am Pharm Assoc (Wash) 1996;NS36(9):565-72
. . . the administration of NSAIDs may lead to loss of intestinal integrity, and contribute to persistence of the disease.
Fries; Journal of Rheumatology, 1991 also stated… • “. . . it generally has been believed that serious complications from NSAID use are very rare and that these familiar drugs are quite safe.” • “Only recently, however has the overall toxicity of NSAID’s been accurately quantitated and the existence of a substantial public health problem identified.” Fries, JF. NSAID gastropathy: the second most deadly rheumatic disease? Epidemioloy and risk appraisal. J Rheumatol 1991; (suppl 28)18:6-10
Understanding Inflammation http://www.arthritis.co.za/cox.html
Pharmacology of Pain • Selective COX-2 inhibitors alleviate inflammation and pain and (in theory) will not cause the side effects associated with COX-1 inhibition (gastric damage, increased bleeding) • The reality is that COX-2 inhibitors do possess some activity against COX-1
New Solutions for Herbal Pain Management • Why treat pain? • Is it valid to consider herbs for treating pain? • The pharmacology of pain (briefly) • Key herbs: California Poppy, Corydalis, Willow Bark • Some major conditions: dysmenorrhea, low back pain, arthritic pain
Pharmacology of Pain • Analgesics are divided into two classes: opiate (opioid) and non-opiate • Morphine and other opiate analgesics stimulate opiate receptors in the CNS and inhibit the perception of pain • Non-opiate analgesics inhibit the manufacture of chemicals that sensitize and/or stimulate pain fibers
Pharmacology of Pain Opiate Analgesics • Opiate analgesics are more effective for the sharp pain associated with the direct mechanical stimulation of pain fibers • They include morphine, codeine and related drugs • They are generally used to relieve intense pain
Pharmacology of Pain Non-opiate Analgesics • Non-opiate analgesics are effective for alleviating the dull throbbing pain associated with such pathological processes as inflammation • They do not relieve the sharp pain associated with direct mechanical stimulation of pain fibers • They are (with the exception of acetominophen) anti-inflammatory agents
Is there a safer and more effective approach? • Nutrition can Influence fatty acid metabolism and eicosanoid synthesis. • Nutrition canmodulate the inflammatory response (suppressing excessively can impair healing). • Nutrition can reduce pain and inflammation without eliminating the benefits of the inflammatory response.
Some Key Analgesic Herbs • California poppy and Corydalis can be seen as opioid-like analgesic herbs. However, their activity is likely to be very mild. • Willow bark can be likened to NSAIDs in its uses • Boswellia, ginger and turmeric are more anti-inflammatory and probably have little analgesic activity • Cramp bark and wild yam for cramping pain in hollow organs
Boswellia Serrata – (Frankincense) • Boswellia is a moderate to large branching tree found in the dry hilly areas of India. When the tree trunk is tapped, a gummy oleoresin is exuded. A purified extract of this resin is used in modern herbal preparations. http://www.virtualhealthinfo.com/herb/boswellia.htm
Boswellia Complex • The gum-resin is reported to possess, sedative and marked analgesic activity. The defatted extract of the gum exudate (oleo-gum-resin) was found to possess marked anti-inflammatory and anti-arthritic activity against adjuvant arthritis in experimental animals and was free from toxicity or any other side effects. • Boswellia reduces the formation of inflammatory leukotrienes by inhibiting 5-lipoxygenase.
Celery Seed • Celery Seed is traditionally used for arthritis, and clears acidic metabolites from the kidneys • Celery has large amounts of potassium and organic sodium that help to rid the body of waste material by stimulating various sites such as the skin, bowels and kidneys. It re-balances the acid/alkaline in the system and may help prevent certain cancers. http://www.healthandage.com/html/res/com/ConsHerbs/CelerySeedch.html
www.csdl.tamu.edu Ginger (Zingiber officinale) …it has been found that ginger alters arachidonic acid metabolism by inhibiting thromboxane synthetase, a pro-inflammatory eicosanoid. Backon J. Ginger: Inhibition of thromboxane synthetase and stimulation of prostacyclin: revelance for medicine and psychiatry. Med Hyp 1986;20:271-8
Turmeric • Anti-Inflammatory Activity http://www.mardi.my/bdc/herba/english/Tumeric.html
Turmeric • A long and storied history for this ginger-looking, brown-on-the-outside, bright-orange-on-the-inside rhizome. It was listed as a coloring agent in an Assyrian herbal dating back to 600 BCE. It was used in sacrificial and religious rites in ancient India and China--and is used likewise to this day. In 1280, Marco Polo mentioned in his journals that he saw turmeric growing in the Fukien region of China, "...a vegetable that has all the properties of true saffron, as well the smell as the color, and yet it is not really saffron."
Boswellia Complex“Natural Anti-Inflammatory” • Each serving contains: • Boswellia gum resin 4:1 extract from Boswellia serrata gum resin 1.2 g Containing boswellic acids 180 mg 300 mg • Celery Seed fruit 6:1 extractfrom Apium graveolens fruit 1.0 g 166.7 mg • Ginger rhizome 5:1 extract from Zingiber officinale rhizome 300 mg 60 mg • Turmeric rhizome 25:1 extract from Curcuma longa rhizome 2.0 g Containing curcuminoids 70.4 mg 80 mg • 4%*
Dosage for Boswellia Complex • 2 Tablets every 2 hours until pain diminishes, then 2 tablets, 3 times per day until bottle is empty.
Side Note-Glucosamine Synergy • While we will discuss the use of Willow Bark, it must be stated that often Glucosamine Sulfate has been beneficial in re-hydrating the chondrocytes of the cartilage and in giving great pain relief. • “Glucosamine synergy”
Willow Bark Extract • The use of willow bark dates back to the time of Hippocrates (400 BC) when patients were advised to chew on the bark to reduce fever and inflammation.
Willow Bark • Many Salix species are used therapeutically especially Salix alba, S. daphnoides and S. purpurea • They all contain derivatives of salicylic acid, mainly salicin • Recent clinical trials have found that a high potency willow bark extract has significant analgesic activity, but with fewer side effects than conventional NSAIDs
The Differing Pharmacologies of the Salicylate Derivatives Salicin • Salicin effectively delivers salicylic acid into the bloodstream, but it does this in a unique way • Salicin is carried unchanged (and hence is stomach friendly) to the distal ileum or colon where gut flora remove the sugar and convert it into salicyl alcohol • The salicyl alcohol is absorbed and oxidized in the blood, tissue and liver to give salicylic acid
The Differing Pharmacologies of the Salicylate Derivatives Aspirin • Aspirin is a potent inhibitor of COX-1 and COX-2 • The acetyl group causes irreversible acetylation of COX which inactivates it • Aspirin therefore has potent analgesic and anti-inflammatory activities (COX-2) but also can cause gastric damage and inhibits platelet function (COX-1)
The Differing Pharmacologies of the Salicylate Derivatives • Platelet function is inhibited by the inhibition of production of thromboxane A2 (a prostaglandin) by COX-1 • Because aspirin irreversibly inactivates COX by acetylation and because platelets cannot make new proteins such as COX (no nucleus) the effect of aspirin persists for the life of the platelet (7 to 10 days)
The Differing Pharmacologies of the Salicylate Derivatives Salicylic Acid • Unlike aspirin, salicylic acid has virtually no inhibitory effect on isolated COX-1 or COX-2 • However it can inhibit PG synthesis in intact cells • This means that salicylic acid or sodium salicylate will have little antiplatelet (blood thinning) effects – they lack the acetyl group
The Differing Pharmacologies of the Salicylate Derivatives • Recently, it has been reported that aspirin and sodium salicylate equipotently suppress COX-2 induction at therapeutic concentrations • Also salicylates appear to have direct analgesic effects in the CNS by unknown mechanisms
Willow Bark More Than Just Salicylate • A study involving 10 healthy volunteers found that a dose of a high potency willow bark extract (providing 240 mg/day of salicin) resulted in blood salicylate levels of around 1.4 g/mL • In contrast, blood salicylate levels of 35 to 50 g/mL have been reported after taking just 500 mg of aspirin • Clearly the clinically-observed analgesic effects from willow bark (see later) must come from more than just the effects of salicylate
Willow Bark • Based on research on willow bark and related herbs it has been suggested that lipoxygenase and hyaluronidase inhibition and free radical scavenging effects, all from other components in willow bark, contribute to the overall analgesic effect • This means that many of the side effects, interactions and contraindications for aspirin, such as interactions with methotrexate, spironolactone and frusemide, are unlikely to apply for willow bark
Willow Bark Clinical Trials Osteoarthritis • In 78 patients with OA of knee and/or hip • Potent willow bark extract (containing 240 mg of salicin per day) versus placebo under double-blind conditions • The WOMAC pain index, (Western Ontario McMaster Universities Osteoarthritis Index ), was used as the outcome after 2 weeks • It dropped by 14% for willow bark versus an increase of 2% for placebo (difference, p<0.05)
Willow Bark Clinical Trials Chronic Low Back Pain • This was a landmark study completed by 191 patients (there were an additional 19 dropouts, mostly in the placebo group) • Under double-blind conditions two doses of willow bark extract (containing 120 or 240 mg of salicin per day) were compared against a placebo • Tramadol was the rescue medication
Willow Bark Clinical Trials • After 4 weeks the number of pain-free patients was an amazing 39% for the higher dose group and 21% for the lower dose group, versus only 6% for placebo • A significant response in the higher dose group was evident after only one week of treatment
Willow Bark Clinical Trials Versus Vioxx in Low Back Pain • An open, randomized, controlled trial compared willow bark extract (containing 240 mg/day salicin) and rofecoxib (Vioxx, 12.5 mg/day) • 114 patients experiencing acute exacerbations of chronic low back pain • After 4 weeks there was no difference observed between the results of the two products in terms of pain, requirement for additional analgesics or side effects
Willow Bark - Matching the Trial Results • In all the trials a high potency willow bark extract was used • The amount of extract was around 400 mg per tablet, standardized to 15% salicin • 2 to 4 tablets per day were prescribed (containing 120 to 240 mg/day salicin) • 400 mg of extract containing 15% salicin corresponds to 6 to 8 g of willow bark, depending on the species used