Download
1 / 45
470 likes | 650 Vues
Case Management for ESRD Patients. Susan Moore, RN, MHSA Managed Healthcare Resources, Inc. Objectives. Identify problems particular to renal case management Determine effective strategies for effective case management Identify how to meet NCQA standards while performing CM duties.

E N D
Case Management for ESRD Patients Susan Moore, RN, MHSA Managed Healthcare Resources, Inc.
Objectives • Identify problems particular to renal case management • Determine effective strategies for effective case management • Identify how to meet NCQA standards while performing CM duties
Definition of Case Management • “A collaborative process which assesses, plans, implements, coordinates, monitors, and evaluates the options and services to meet the individual’s needs using communication and available resources to promote quality cost effective outcomes.” • “A system with many elements: health assessment, planning, procurement, delivery and coordination of services, and monitoring to assure that the multiple service needs of the client are met.”
What is Case Management? • Definition: • A system by which one professional is responsible for assuring that a patient receives a full spectrum of services required • A case manager acts as a broker to arrange both hospital and community services • Case management includes: • comprehensive assessment of needs and resources, development of a care plan, referral follow-up, and periodic evaluation of the plan
Case Management Objectives • Depend on: • the organization’s perspective and the design of the case management system • the population served and its health status • the type of case management allowed or offered by an organization • the case manager’s level of expertise • the method by which case management is linked to the organization
Benefits of Case Management • Increased satisfaction of patients and families • Fits well with the principles of managed care • Effective cost containment strategy • Well-suited for use across the full continuum of care
Why case management with ESRD? • High cost – over $14,000 per month • Prone to high ER and hospitalization use • Disease involves multiple systems • High amount of co-morbidities (those with diabetes and CHF have much higher hospitalizations, and CHF 37% higher than diabetes)
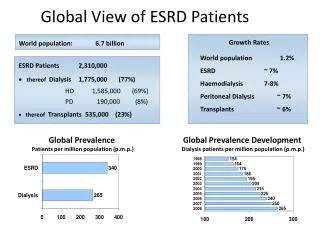
Burden of disease in U.S. • Rising incidence and prevalence of kidney disease at all stages – ESRD doubled in last 10 years • 4% of the U.S. population (8 million people) have moderate to severe CKD • Expected to increase with hypertension and diabetes and aging population • Expected at 2015 to increase from 450,000 ESRD now to 600,000
Cost of ESRD • In 2003, ESRD cost private insurers and Medicare more than $27 billion and was 6% of entire Medicare expenditures ($9 billion absorbed by private insurers)1 • Annual cost averages $60,000, with highest cost the year of initiation of dialysis2 • Dialysis 2.8 times more costly than transplant3 • 1AmJ KidneyDis, 2003, 41 • 2J Am Soc Nephrol., 2005, 16 • 3Report to the Congress: New Approaches in Medicare, June 2004
Impact • Those under 65, Medicare begins after 3 months on dialysis UNLESS… • They have private insurance, then Medicare begins after 33 months on dialysis • Analysis for CKD progression (before ESRD) estimated that if GFR decreased by only 10% per person, almost $20 billion could be saved in 10 years3 • Nearly 45% of ESRD attributable to diabetes and 20% to chronic hypertension4 • 3, 4Journal of Managed Care Pharmacy, April 2007
Utilization • Between 1993 and 2001, rates of hospitalization per 1,000 patient years ranged from 2,019 to 2,0625 • CKD – Earlier referral to a renal team before ESRD led to lower risk of unplanned first dialysis, fewer complications, lower hospital costs and shorter durations of hospitalization in first 3 months of dialysis, likelier to have mature A-V fistulas (only 29% had in 2001, and 90% need) 6 • 5,6Report to the Congress: New Approaches in Medicare, June 2004
Impact of case management on ESRD • Health plans with disease management programs for ESRD had: • 19 – 35% better survival rates than FFS Medicare ESRD • 45 – 54% fewer hospitalizations than FFS Medicare ESRD7 • 7Report to the Congress: New Approaches in Medicare, June 2004
Case Management Components • Case identification and eligibility determination • Assessment or evaluation • Care plan development • Implementation or coordination • Follow-up • monitoring • reassessment • discharge
Case Identification Efforts to define and target the desired population* • Claims or encounters – dialysis revenue codes of 0821, 0831, 0841, 0851 • Hospital discharge data • Pharmacy data – aluminum hydroxide (Alucaps), calcium carbonate (Calcichew, Titralac), calcium acetate (Phosex), lanthanum carbonate (Fosrenol), Sevelamer (Renagel) • Data collected through the UM process *2007 NCQA QI 7 Element A
Access to Case Management* • Health information line referral • DM program referral • Discharge planner referral • UM referral • Member self-referral • Practitioner referral *2007 NCQA QI 7 Element B
IT support* Case management systems should support: • Using evidence-based guidelines to conduct assessments • Automatic documentation of date, time, and individual for actions/patient interactions • Automated prompts for follow-ups *2007 NCQA QI 7 Element C
Assessment Determines the needs and provides information to develop an individual care plan • may be conducted by an individual case manager (e.g., social worker or nurse) or by a multidisciplinary team • goal is to obtain a complete view of the individual and their circumstances
Initial Assessment* • Member’s health status, including disease-specific issues • Clinical history, including medications • Activities of daily living • Mental health status, including cognitive function • Evaluation of cultural and linguistic needs, preferences or limitations • Evaluation of caregiver resources • Evaluation of available benefits • Assessment of life planning activities *2007 NCQA QI 7 Element E
Medical complications of ESRD and dialysis • Anemia – erythropoeitin not produced in kidney • Bone disease – calcium and phosphorus imbalance • Hypertension – primary disease, fluid retention • Fluid overload – little to no output of kidneys • Pericardial effusion and pericarditis – inadequate dialysis, fluid overload, and infection • Hyperkalemia – inadequate dialysis and noncompliance with dietary restrictions • Peripheral neuropathy – uremic toxins • Infection of vascular access
Physical issues with ESRD patients • Fatigue – secondary to anemia • Itching – phosphorus • Vascular access patency • Sleep disorders • Pain and restless legs
Emotional/psychosocial issues • Change in social position/role in family • Marital problems • Employment – loss of • Impaired libido and impotency • Diet • Compliance or motivation to comply • Appearance and clothing restrictions • Frequent loss of independence and control • Depression (upwards of 40%) and anxiety • Reported increased incidence of cocaine, heroin, and methamphetamine use
Additional factors • Age • Social or ethnic background and response to illness • Recent other life crises • Personality of the patient • Psychiatric history of the patient and family • Cognitive ability of the patient and family
Special issues for Medicaid • Homelessness or group homes • Drug abuse • Transportation needs • Mental health issues • Greater problems with missing dialysis treatments
Reasons for ER or hospitalization • Clotted access (decreased inpatient 24% as these have moved outpatient) • Infection – due to catheter use, up 23% in last 10 years • CHF due to fluid overload/anemia • Cardiomyopathy • Hyperkalemia • Hypertension • Co-morbid conditions
Care Plan* • Development of short and long term goals • Identification of barriers to meeting goals or compliance with plans • Development of schedules for follow up and communication with members • Development and communication of self-management plans for members • Assessment of progress against case management plans and goals and modification as necessary *2007 NCQA QI 7 Element F
Care Plan • Developed to address the needs and problems identified in the assessment • includes agreement with the individual and involved family members on goals and priorities • outlines the problems,type and level of assistance needed, the roles of the patient/client and family who will provide the services and desired outcomes • knowledge of service options, local resources, delivery systems, qualified providers, financial alternatives, available benefits, and eligibility requirements for assistance are critical to the plan
Important issues for case managers • Maintaining confidentiality, patient rights, and privacy • Building relationships with MSWs and nurse managers at dialysis units • On-site or telephonic case management…..
Telephonic Less intrusive Less expensive On-site More intrusive Less likely to misconstrue objective of case management See patient and develop a relationship More coordination with the dialysis team Telephonic vs. On-site?
Who’s on the dialysis team? • Renal social worker (MSW) • Nephrologist • Nephrology nurses • Renal technologists • Patient care technicians • Dieticians • Financial counselor (sometimes)
Role of the renal social worker • Initial assessment and intervention • Crisis counseling • Linkage with local, state, and federal resources • Assistance with Medicare application • Assisting the patient and family in adjusting to dialysis and ESRD • Promotion of independence • Identification of needs in the home • Mediating staff/patient conflicts
Teaching needs (by dialysis team or case manager) • ESRD • Diet and fluid restrictions • Vascular access • Drugs
Diet • Limited in phosphorus, potassium, sodium, and fluid • Processed meat and cheese, dried fruit, beans, peanut butter, and eggs are high in phosphorus • Challenge is to obtain enough protein and calories to prevent cell breakdown • More challenging with diabetes and other dietary restrictions, such as low fat for heart disease
Drugs – phosphate binders • Types: • Calcium carbonate • Calcium acetate (PhosLo - $0.20/pill) • Sevalamer hydrochloride (RenaGel -$1.50/pill) • Lanthanum carbonate (Fosrenol - $2/pill) • Noncompliance is common (frequently due to forgetting) • In the Dialysis Outcome Study, fewer than 50% met the guideline recommendations for phosphorus control
Problems that occur during hemodialysis • Cramping – due to volume changes • Hypotension – ultrafiltration with inadequate vascular refilling • Arrhythmias – fluid and electrolyte changes • Hypoxemia – in 90% of patients, pO2 drops 5 – 35 mm Hg. • Hemolysis – biochemical and toxic insults. Half life of RBC is ½ to ⅓ of normal RBCs.
Issues typically addressed by dialysis team • Anemia • Depression • Noncompliance
Anemia • Goal: keep Hgb. 11 – 12 gms/deciliter • Iron levels are monitored and iron given IV • Epogen given to combat anemia, but inappropriate use increases mortality • Anemia can lead to LVH and CHF
Depression • Actual clinical depression high • Interferes with compliance with treatment regimen • Identify when patients may be ready to give up – withdrawal from dialysis occurs in about 20% of dialysis patients before their death • Encourage evaluation by behavioral health, PCP, or nephrologist for an SSRI
Dealing with noncompliance • Many reasons for noncompliance • Execute a contract with the patient • Work with the dialysis social worker • Meet with family, if possible • Refer to behavioral health as necessary • Communicate with PCP/nephrologist
Do you discharge from CM? • If patient is stable • Verbalizes understanding of disease process(es) and care of access • If no unnecessary hospitalizations or ER visits • Compliant with medications, diet, and dialysis regimen • Not depressed
Keys to effective case management • Identify all of the main problems at the initial assessment • Intervene very frequently initially to make sure you address all the key issues • Keep your eyes on the care plan as you go along and update it as frequently as necessary
Keys to effective case management (cont.) • Perform intermittent assessments for long term clients, because things change • Develop relationships with the dialysis personnel and the nephrologist or PCP • Remember preventive measures (immunizations, mammograms and cervical cancer screenings, condition-specific HEDIS measures)
Evaluation of case management* Selection of three measures to evaluate effectiveness that are: • A relevant process or outcome • A valid method with a quantitative result • Set a performance goal • Clear specifications • Analyze results • Identifies opportunities for improvement • Develops plan for intervention and remeasurement *2007 NCQA QI 7 Element G, H
Evaluation of successful ESRD case management* • Lower costs • Lower ER visits per 1,000 • Lower inpatient stays per 1,000 • Higher patient satisfaction • Potential higher quality of life (QOL) scores
So what about all this information? We’ll apply the information from the first presentation and this presentation to the case studies to follow.
Resources Those wanting any of the documents used for background data used for the presentation, please feel free to email me at skmoore627@comcast.net Nephronline.com is a free registration for periodicals