Download
1 / 50
530 likes | 815 Vues
Early Intervention Options for Infants and Toddlers with Hearing Loss. A. Brancia Maxon, Ph.D. T. Foust, Au.D. R. Winston, M.A. K. Ditty, M.S. P. Martin, Ph.D. National Center for Hearing Assessment and Management. UNHS and Early Intervention.

E N D
Early Intervention Options for Infants and Toddlers with Hearing Loss A. Brancia Maxon, Ph.D. T. Foust, Au.D. R. Winston, M.A. K. Ditty, M.S. P. Martin, Ph.D. National Center for Hearing Assessment and Management
UNHS and Early Intervention • Universal newborn hearing screening has resulted in • decreased age of identification • decreased age of diagnosis • decreased age of amplification fitting
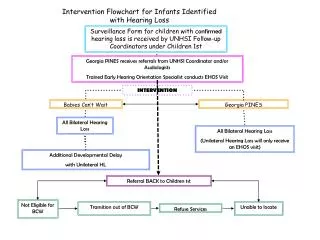
Ultimate Goal of UNHS • Primary purpose of UNHS is to ensure that • these very young children and their families are enrolled in EI services within first few months of life • EI services are appropriate for the varied and extensive needs of infants with hearing loss and their families.
Early Intervention Benchmarks • Infants enrolled in family-centered EI by 6 months old • Infants enrolled in family-centered EI program with professionals knowledgeable about communication needs of infants with hearing loss • Amplification use begins within one month of diagnosis when appropriate and agreed on by family JCIH, 2000
Early Intervention Benchmarks • Infants with hearing loss have ongoing audiological management - not to exceed 3 month intervals • Language development in family’s chosen communication modality and commensurate with developmental level and similar to that for hearing peers of a comparable developmental age. • Families participate in and express satisfaction with self-advocacy. JCIH, 2000
Principles of Intervention for Infants and Toddlers with Hearing Loss • Ongoing audiological assessment and management must be conducted by staff trained to work with infants and young children. • The intervention team should assist the family in learning about the nature of their child’s hearing loss.
Principles of Intervention for Infants and Toddlers with Hearing Loss • Intervention requires a team approach. • family is the most important member of this team • team supports, assists and advises families on how to best meet child’s unique needs • team provides family with access to a wide variety of information that is shared in an unbiased manner.
Principles of Intervention for Infants and Toddlers with Hearing Loss • Parents and children are partners in communication. • Parents and children develop a communication system so a language system can develop. • Language acquisition begins at birth and develops through interactions with the family in daily routines.
Principles of Intervention for Infants and Toddlers with Hearing Loss • EI program helps parents understand, manage and maintain amplification or other sensory devices. • EI program helps parents understand their legal rights so they may advocate for their child. • EI should take place in natural environment (Part C IDEA - U.S.)
Principles of Intervention for Infants and Toddlers with Hearing Loss • These are achievable goals • Practical implementation affected by cultural, geographic, linguistic and socioeconomic factors
Information for IFSP • Moderate to Profound Hearing Loss • Medical Intervention • Medical clearance for hearing aids • Monitoring for middle ear problems • Genetic assessment and counseling . (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Moderate to Profound Hearing Loss • Audiological Intervention • Amplification selection, fitting, validation • Audiological evaluation at least every 3 months • Monitoring hearing levels for any change • focus on residual hearing • amplification use • speech and language development • consider communication modality (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Moderate to Profound Hearing Loss • Communication Intervention • Speech and language development • Listening development • Direct service • Bombard with vocabulary, correct structures and speech sounds (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Mild Hearing Loss • Medical Intervention • Medical clearance for hearing aids • Monitoring for middle ear problems • Genetic assessment and counseling (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Mild Hearing Loss • Audiological Intervention • Amplification selection, fitting, validation • Audiological evaluation at least every 3 months • Monitoring hearing levels for any change (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Mild Hearing Loss • Communication Intervention • Speech and language development • Stimulate consonant production – especially unvoiced sounds • Reinforce all vocal attempts • Listening development • Expect and wait for searching response to speech (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Mild Hearing Loss • Communication Intervention • Speech and language development • Stimulate consonant production – especially unvoiced sounds • Reinforce all vocal attempts • Listening development • Expect and wait for searching response to speech (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Mild Hearing Loss • Parent Education • Modeling stimulation techniques • Facilitating carry over of mastered skills • Use of daily routines for communication development • Need for full-time amplification • Difficult listening conditions (Brackett, Maxon and Blackwell, 1993)
Issues in EI resulting from UNHS • Mild losses • Parent expectations • Speaking – length of time between enrollment and first words • hearing – must be convinced of importance of keeping on hearing aids • Professional expectations • Knowledge of very early communication development
Information for IFSP • Unilateral Hearing Loss – Medical Intervention • Monitoring for middle ear problems • Genetic assessment and counseling (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Unilateral Hearing Loss • Audiological Intervention • Audiological evaluation at least every 3 months • Monitoring hearing levels for any change in normal ear • Determine if amplification and/or sound field FM is beneficial • Determine listening environment effects in all daily living situations (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Unilateral Hearing Loss • Communication Intervention • Monitoring speech and language development • Monitoring listening development (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Unilateral Hearing Loss • Parent Education • Use of daily routines for communication development • Establishing good listening conditions • Situating the child’s good ear appropriately • Use of amplification when appropriate (Brackett, Maxon and Blackwell, 1993)
Issues in EI resulting from UNHS • Unilateral Hearing Losses • 35 to 48% of sensorineural hearing losses are unilateral • Unilateral hearing loss has significant effects • average percentage: 25% language 30% math 32% social
Issues in EI resulting from UNHS • Unilateral Hearing Losses • Parent expectations • Hearing: the child reacts to most sounds including speech and environmental • difficult to understand potential negative outcomes • Communication: minimal differences when compared to infants with normal hearing • difficult to understand potential negative outcomes • Professional expectations • Effects of difficult listening on hearing
Information for IFSP • Conductive Hearing Loss • Medical Intervention • Medical treatment of middle ear disease is critical • Fluid may continue and need pressure equalizing tubes (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Conductive Hearing Loss • Audiological Intervention • Ongoing audiological evaluation • Monitoring hearing levels with and without fluid • Determine listening environment effects in all daily living situations (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Conductive Hearing Loss • Communication Intervention • Monitoring speech and language development • Monitoring listening development • Increasing caregiver input • Employing vocal play • Stimulating consonant production • Expect and wait for responses to speech • Reinforce all vocal attempts (Brackett, Maxon and Blackwell, 1993)
Information for IFSP • Conductive Hearing Loss • Parent Education • Model techniques for enhancing vocal play • Establishing ways to increase input during daily routines (Brackett, Maxon and Blackwell, 1993)
Issues in EI resulting from UNHS • Conductive Hearing Losses • Parent expectations • hearing – separating medical and auditory issues • communication – changes in hearing result in potential effect on speech and language development • Professional expectations • Working closely with physicians
Parent Perceptions of EI • At diagnosis • parents wanted to know cause of the hearing loss regardless of degree of loss their child had. • Parents of children with milder degrees of hearing loss preferred to have more educational information • e.g., understanding the audiogram • Parents of children with severe to profound losses wanted emotional support. (Harrison and Roush, 2004)
Parent Perceptions of EI • Later in early intervention • parents wanted to know about how their child was going to learn to speak and use hearing. • Parents of children with milder losses wanted to know about timelines and early intervention • Parents of children with severe to profound losses were interested in cochlear implants (Harrison and Roush, 2004)
Parent Perceptions of EI • The benefits of amplification are important to parents. • almost 70% of parents interviewed questioned the benefit of the hearing aids their child was using. • less than 15% felt their child’s performance with the hearing aids met their expectations. (Sjobad, et al, 2004)
Parent Perceptions of EI • This may have occurred because parents were not well informed about hearing aids and their benefit. • Need to be sure the child’s hearing aids were appropriately fit. • Concerns about damaging the child’s residual hearing may result in under amplification and poor auditory responses. • Therefore, the parents will not see what they expect. (Sjobad, et al, 2004)
Early Intervention and continuous early childhood hearing screening
The Hearing Head Start Project From2001 – 2004, NCHAM conducted a pilot project helping early intervention programs. . . • Migrant Head Start • American Indian Head Start • Early Head Start . . . update hearing screening practices for children 0 - 3 years of age using OAE technology.
As many as 50% of infants who refer from newborn hearing screening are lost to follow-up. Hearing loss can occur at any time in a child’s life. Approximately 35% of preschool children will have repeated ear infections before 3 years of age, sometimes resulting in fluctuating conductive hearing loss. Without regular, physiologic screening, hearing loss is often impossible to detect. Why is Continuous Hearing Screening so Important?
OAE Screening/Referral Outcomes 3487 children screened (using a 3 - step screening protocol) 181 (5%) were referred for medical/audiological follow-up • 17 identified with hearing loss • 53 identified with outer or middle ear disorder requiring medical or surgical intervention • 18 normal • 82 exited program or parent refused follow-up
Native American Populations:Considerations In Providing Quality EI • The foundation for successful EI is respect for the native way of life and their traditions • Treat the child as a “whole” person • Incorporate culturally receptive materials
Native American Populations:Considerations In Providing Quality EI • Appreciate importance of the family structure and their strong connection to their community • Collaborate and partner with other programs and services • Guide families through the system
Rural Area + Low SES: EI Realities • Difficult to achieve “buy-in” regarding family-centered care • Cultural mismatch • Invasiveness • Religious influence • Day-to-day existence
Rural Area + Low SES: EI Realities • Other contributing factors • low literacy levels of families • lack of transportation to services • lack of trained providers • non - English speaking families, finding materials in family language working through a translator • funding sources
Cultural Diversity • Gender, race, religion, ethnicity, language, income, and age are all factors to be considered in developing Early Intervention strategies
Cultural Diversity • A growing number of children • with hearing loss in the United • States are from families that are • made up of non-native English • speaking. • The 2000 U.S. Census shows • that nearly one out of five • Americans speak a language • other than English at home.
Cultural Diversity • Informational materials should be provided in native languages for parents and at understandable reading levels. • Communication options chosen by families for their child should be respected and supported.
Cultural Diversity • Alberg and Kerr (2004) developed a list of considerations for service providers working with multicultural populations. • Families are more comfortable with service providers who speak their language and understand their culture. • Printed material should be available in the language of the client base. • There may be different dialects among people from the same country.
Cultural Diversity • Racial, cultural and socioeconomic differences may exist among individuals from the same country. • Interpreters may have difficulty explaining medical and technical information • May be difficult for the family to understand. • Families sometimes enter the U.S. illegally. • will not qualify for public assistance medical and technical services (e.g., hearing aids) • finding financial assistance for these families is challenging, at best
Home visits - Issues • Respect the home environment (shoes) • Accept offers of hospitality (coffee, food) • Feel comfortable working in the home (cleanliness, animals) • Dress appropriately for the environment (sitting on the floor) • Be on time (arrival and departure) • Integrate family into the sessions
Summary • EI services can be conducted in a variety of settings • EI services can meet the needs of all infants/toddlers with hearing loss and their families