TRIAGE
TRIAGE. Goals of Triage. Rapidly identify patients with urgent, life-threatening conditions Assess/determine severity and acuity of the presenting problem Direct patients to appropriate treatment areas Re-evaluate patients awaiting treatment. Advantages of Triage. Streamlines patient flow.


TRIAGE
E N D
Presentation Transcript
Goals of Triage • Rapidly identify patients with urgent, life-threatening conditions • Assess/determine severity and acuity of the presenting problem • Direct patients to appropriate treatment areas • Re-evaluate patients awaiting treatment
Advantages of Triage • Streamlines patient flow. • Reduces risk of further injury/deterioration. • Improves communication and public relations. • Enhances teamwork. • Identifies resource requirements. • Establishes national benchmarks.
Triage Acuity Determinants • Chief complaint. • Brief triage history. Injury or illness(signs & symptoms). • General appearance. • Vital signs. • Brief physical appraisal at triage.
Triage Role • To determine severity of illness or injury for each patient who enters the Emergency Department (ED).
Triage • Patients should have a triage assessment within 10 minutes of arrival in the ED. • Accurate triage is the key to the efficient operation of an emergency department. • Effective triage is based on the knowledge, skills and attitudes of the triage staff.
Triage Process • Assess and determine the severity or acuity of the presenting problem. • Process the patient into a triage level. • Determine and direct the patient to appropriate treatment areas. • Effectively and efficiently assign appropriate human health resources.
Triage Assessment • Chief complaint. • Brief triage history Injury or illness (signs & symptoms) • General appearance. • Vital signs. • Brief physical appraisal at triage.
5 Level Triage • Level 1 Resuscitative • Level 2 Emergent • Level 3 Urgent • Level 4 Less urgent • Level 5 Non-urgent
Triage is a dynamic process. • Reassessment & Reassessment . • A patient’s condition may improve or deteriorate during the wait for treatment.
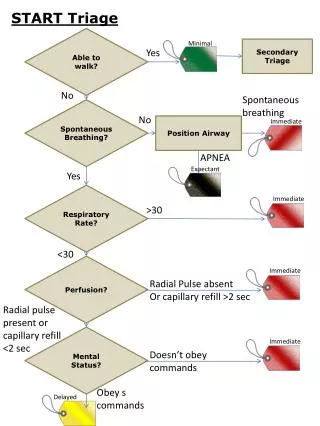
Level I: Resuscitative • Conditions that are threats to LIFE or LIMB (or imminent risk of deterioration) requiring aggressive interventions. • Time to MD: Immediate • Time to Nurse: Immediate • Continuous reassessment
Level I • Usual presentations • Code / arrest. • Major trauma. Severe burns--airway compromise . • Shock states. • Severe respiratory distress. Near death asthma (Status asthmatics). Tension pneumothorax. • Altered mental state. • Seizure (Status epileptics). • Traumatic shock. • Overdose. • AAA. • AMI with complications. • Congestive heart failure with low BP. • Major head injury-unconscious.
Level II Emergent • Conditions that are a potential threat of life, limb or function, requiring rapid medical intervention or delegated acts. • Time to MD: 15 minutes. • Time to Nurse: immediate. • Reassessment time: 15 minutes.
Level II Emergent • Usual presentation • Chest Pain Query MI • Trauma • Chemical Exposure • Stroke • Altered Consciousness • Acute MI • Severe Asthma-stridor • Acute Psychotic Episode with Agitation • Severe Pain 8 -10 • Reassessment 15 mins
Level III Urgent • Conditions that could potentially progress to a serious problem requiring emergency intervention. • May be associated with significant discomfort or affecting ability to function at work or activities of daily living. • Time to MD: <30 minutes. • Time to Nurse: 30 minutes. • Reassessment time: 30 minutes
Level III Urgent • Usual presentations: • Renal colic, billary colic • GI bleed with normal VS • Previous seizure—alert • Dehydration. • Shunt dysfunction. • Vital signs outside normal range. • Pain scale 4 -7 \10 • Moderate risk of harm to self or others. • Inconsolable infant , infant not feeding. • Behavior change. Reassessment 30 minutes
Level IV: Less Urgent • Conditions that related to patient age, distress, or potential for deterioration or complications would benefit from intervention or reassurance within (1 –2 hours) • Time to MD < 60 minutes (1 hr) • Time to Nurse < 60 minutes (1 hr) • Reassessment time: 60 minutes (1 hr)
Level IV: Less Urgent • Usual presentation: • Head injury—alert. • Earache. • Abdominal pain. • UTI sign and symptoms. • Simple laceration requiring sutures. • VS normal • Reassessment 1 hour
Level 5: Non Urgent • Conditions that may be acute but non-urgent as well as conditions which may be part of a chronic problem with or without evidence of deterioration. • The investigation or interventions could be delayed or even referred to other area of the hospital or health care system. • Time to MD: 120 minutes. • Time to Nurse: 120 minutes. • Reassessment time: 120 minutes
Level 5: Non Urgent • Usual presentation: • Strains. • Sprains. • Single episode of vomiting. • Sore throat. • Script refills. • Chronic problems with no change. • Investigation or intervention for these illnesses or injuries could be delayed or even deferred. • Reassessment 2 hours \120 minutes
Pediatric Triage PCTAS • There are three things that must be assessed and documented on all pediatric patients: • Respiratory rate. • Heart rate. • Capillary refill.
Pediatric Vital Signs • Must include: • Heart rate. • Blood pressure. • Respiratory rate. • O2 saturation. • Temperature. • Capillary refill. • Accurate weight!
Vitals Are Your Safety Net. • Less Urgent and Non Urgent patients have NORMAL vital signs. • Abnormal vital signs are at least an URGENT.
Triage is a dynamic process • A patients condition may improve or deteriorate during the waiting for treatment • Reassessment, Reassessment, Reassessment
General Approach toPOISONED Patient • ABCs…IV, O2, monitor • Decontaminate if organophosphates prior touching by health care professionals • Lily kit for cyanide poisoning. • History • Obtain all prescription and bottles in the household (call pharmacy). • Pill count. • PM Hx. • Search clothes for clues, medication alerts, pills etc. • Contact family members. • Track marks, consider body packing or stuffing. • Vital signs, Rhythm strip.
General approach to poisoned pt. • What are the essential features of a 30-second toxicological exam? • Vital signs- HR, RR, BP. • Temperature- rectal (resp rate can affect oral temperature). • Skin- color, temperature, and sweating. • Odors- provide clues (their absence means nothing) • Bowel sounds and bladder function. • Mental status.
General approach to poisoned pt • Tests • GI Decontamination • Activated Charcoal • Antidotes