Plasmodium & Malaria: Life cycle
Plasmodium & Malaria: Life cycle. Charles Laveran (1880), for the first time noticed the microbes in the blood of a malarial patient. Sir Ronald Ross(1889), experimentally worked out intermediate host the Plasmodium its modes of transmission
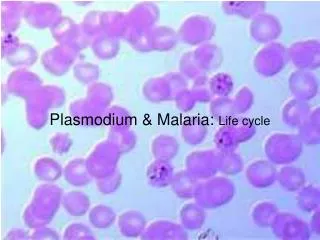

Plasmodium & Malaria: Life cycle
E N D
Presentation Transcript
Charles Laveran (1880), for the first time noticed the microbes in the blood of a malarial patient. Sir Ronald Ross(1889), experimentally worked out intermediate host the Plasmodium its modes of transmission Grassi (1890) provide the proof for the specific relationship with the Anopheles mosquitoes and plasmodium important species cause malaria Plasmodium falciparum, Plasmodium malaria, Plasmodium vivax, Plasmodium ovale.
Plasmodiumis an intracellular sporozoan blood parasite. Man is the intermediate host and the mosquito is the definitive host. In man its reproductive mode is asexual and in mosquitoes it is sexual. Female Anopheles mosquitoes inoculates the plasmodium in the form of spindle shaped sporozoites in the human blood. Classification: Phylum : Protozoa . Class : Sporozoa . Order : Haemosporidia .
Plasmodium: Life cycle in Man - Schizogony The two phases in the life cycle of plasmodium: Pre erythrocytic or Exo erythrocytic cycle (in liver cells) Erythrocytic cycle or Endo-erythrocytic cycle (inside RBCs )
Pre Erthrocytic Cycle Myriads of sporozoites are injected in the blood. They first enter the capillaries of the skin and then enter in the general circulation. They circulate in the blood about 30 minutes and sheltered at reticulo-endothelial cells of the liver. At liver cells they develop into forms known as Cryptozoites (which have a compact nucleus and no pigment or vacuoles)
Pre Erthrocytic Cycle Cryptozoites rapidly grow on the liver cells. When it has reached the full growth it fills the entire cell. This stage is known as Crypto-Schizont. This Crypto-schizonts undergoes Schizogony and the resulting cells known as Crypto-Merozoites. The crypto- merozoites are set free in the blood by the rupture of liver cells
Pre Erythrocytic Cycle The released crypto-merozoites invade fresh liver cells and RBCs. This cycle is considered as the period of incubation before the parasites could start the Endo-erythrocytic or erythrocytic cycle During this period of 7-17 days, the parasites are not seen in the blood stream
Erythrocytic (endo-erythrocytic) Cylcle Each cryptomerozoite makes its way into RBCs and feeds on its contents. Then the parasite gets an amoeboid shape. This stage is known as trophozoite stage. Trophozoite develops a vacuole which increases its size. Thus the nucleus is pushed to one end. This stage is called the Signet ring stage. With further growth vacuole disappears and the amoebula occupies entire corpuscle. This stage is known as schizont stage.
Erythrocytic (endo-erythrocytic) Cylcle In the Schizont, the nucleus breaks up into bits(6-24) and each becomes surrounded by a small cytoplasm. These cells are known as Merozoites Merozoites break the wall of RBcs and penetrates into the blood along with the haemozoin which causes the malarial fever
Erythrocytic (endo-erythrocytic) Cylcle The liberated Merozoites attack another set of RBCs and start the life cycle anew. This method of infection is known as autoinoculation. The life cycle in the human blood is called the Cycle of Golgi or Schizogony or Endoerythocytic cycle. Schizogony keeps up the multiplication of the parasites and their maintenance in the blood. *Schizogony *
«¸îº¢ÅôÀÏî ÍÆüº¢ After schizogony has taken palce of several generations some merozoites which invade the RBCs develop into (Micro and Macro) gametocytes. The Macro Gametocyte has a small nucleus and dense food laden cytoplasm. The Micro gametocyte has a relatively large nucleus and clear cytoplasm. Their further development depends on their entry into the stomach of a female anopheles. If it does not take place they distegrate. * ¨º§…¡¸É¢ - Schizogony *
Life cycle in Mosquito - SPOROGONY In the gut of mosquitoes only the mature gametocytes survive and the rest of the stages are destroyed. From the gametocytes develop gametes. The development of gametes from gametocytes is known as gametogony.
GAMETOGONY The nucleus of micro gametocyte divides into many fragments and the cytoplasm is thrown into flagellated structures. There may be as many cytoplasmic structures as there are nuclei. The resultant cells are called the Microgametes. The Macro-gametocyte becomes female gamete or Macrogamete.
Syngamy and Sporogony Inside the stmach of the mosquito the microgamete fuse with the Macrogamete and formed as Zygote. This fusion is called Syngamy. The zygote assumes as an elongated form and is capable of movement. It is known as Ookinete. Ookinete pierces the wall of the stomach and comes to lie under the outer layer of stomach wall. Syngamy and Sporogany
Syngamy and Sporogony Then the Ookinete ceases to move, becomes round and forms a membranous cyst-wall. This zygote enclosed in a cyst-wall is known as Oocyst. Oocysts grow in size absorbing the nourishment from host. The nucleus of the Oocyst divides repeatedly, each being surrounded by a fragment of cytoplasm. Thus inside the Oocyst , a large no.of cells develop into a minute, slender, sickle shaped bodies called Sporozoites.
Syngamy and Sporogony The cyst wall breaks, liberating the sporozoites into the body cavity (haemocoel) of the host. They wriggle forward and enter the salivary gland. When such a infected female anopheles bites a healthy person, it injects into his blood stream of sporozoites. This kind of transmission is called Inoculation.
Malaria • The disease caused by the Plasmodia is known as Malarial fever. It is characterized by recurring bouts of fever, each lasting several hours. • The patient suffers from shaking chills, and sweating. • As the chills subside, the body temp. may rise to 106◦ F. • The high fever is induced by the toxic haemozoin granules. • haemozoin are liberated in plasma when the parasite schizonts bursts out from the RBCs. • The patients also suffers from severe anaemia due to destruction of erythrocytes.
Types of Malaria Tertian, Beningn tertian or Vivax malaria caused by Plasmodium vivax. The fever recurs every 3rd day (every 48 hours) Quartan malaria caused by Plasmodium malariae. The feverish fits every 4th day (every 72 hours) Mild tertian or Ovale malaria caused by Plasmodium ovale. This is widely popular in West Africa occasionally in Russia, Palestine and south America. Malignant Tertian or Pernicius malaria caused by Plasmodium falciparum. This type has high mortality. The parasitised RBCs tend to clump together and block up small blood vessels and damage essential organs. It often appears in epidemic scale. These 4 species differ from each other in the details of structure, time needed to complete the Schizogony, the incubation period, no. of merozoites released and duration of sexual cycle.
Other symptoms of Malaria Enlargement of spleen, due to massive increase in the no. of phagocytes, macrophages of lymphatic system. In the case of falciparum infection the thrombosis of visceral capillaries occurs. Death takes place when the capillaries of brain are plugged with both of parasites and the malarial pigments. Another serious outcome of the falciparum infection is the Black water fever (which is characterized by the mass destruction of patients’ RBCs and the excretion of liberated haemoglobin in the urine.).
Control of Malaria … The malarial control measures … Treatment of infected patient, Prevention of infection, Control of vectors.
Control of Malaria Treatment of infected patient: Malaria can only be treated with drugs that may kill all stages of parasite without poisoning the patient. Quinine (extracted from the bark of Chincona trees) has been used effectively to cure malaria (for the past 300 years) Chloroquin, Camoquin, Pamaquin, Resochin, Atabrin etc.,
Control of Malaria Prevention of infection: It can be effected in two ways, Using the mosquito repellants, Mosquito nets etc., Use of prophylactic drugs; small daily dose of anti-malaria drugs. Control of vectors: It is the useful and effective way of Malarial control. It is achieved by the insecticides, bio-control measures and by draining swamps.