Download
1 / 15
661 likes | 4.89k Vues
Body Weight Support Treadmill Training. Shaun Coffman Kara Fry Candace Kochman Doug Palmer Michael Short Kevin Swank Brooke Vaughan. What is Locomotor Training?.

E N D
Body Weight Support Treadmill Training Shaun Coffman Kara Fry Candace Kochman Doug Palmer Michael Short Kevin Swank Brooke Vaughan
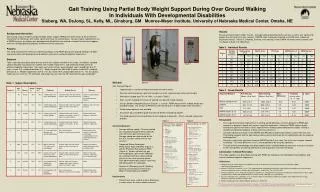
What is Locomotor Training? • Locomotor training is a physiologically based approach to retraining walking after neurological injury which capitalizes on the intrinsic properties of the spinal cord to generate stepping in response to specific afferent input associated with the task of walking (Berhman 2006). • The primary goal of locomotor training is to provide the appropriate sensory input associated with the normal gait cycle. This may be accomplished using either BWSTT or overground locomotion training.
Locomotor Training Focuses on the neuroplasticity of the spinal cord in order to retrain gait patterns Utilizes the relationship between central pattern generators and sensory input Promotes proper gait kinematics Designed to facilitate weight bearing through the lower extremities Allows for longer duration of task-specific practice More equipment and/or therapists may be needed, possibly making training difficult in an outpatient setting Conventional Gait Training Focuses on the remaining musculature and assistive devices in order to achieve ambulation Promotes compensation during gait Use of assistive devices increases weight bearing through the upper extremities which may inhibit rhythmical stepping Duration of practice may be limited due to increased energy demands caused by compensatory strategies Requires less resources, equipment than locomotor training Locomotor Training vs. Conventional Gait Training
Theoretical Model • The current human model for locomotor training is based on previous studies in which spinally transected cats were able to generate hind-limb stepping. • The cats were provided with trunk support and were given manual assistance to ensure proper gait kinematics. After several weeks of training, the cats were able to independently generate stepping motions. Furthermore, the cats were able to respond appropriately to changes in speed by increasing step cadence and length. • Researchers believe this phenomenon is due to the capacity of the spinal cord to integrate the afferent sensory information, interpret it, and produce a coordinated, adaptable locomotor pattern even in the absence of supraspinal influences.
Theoretical Model • Researchers believe that the ability of the spinal cord to generate rhythmical movements in the absence of supraspinal influence is due to the presence of central pattern generators (CPGs). • The exact make-up or location of CPGs is not known, but they appear to consist of networks of interneurons between contralateral lower extremity (LE) flexor and extensor muscle groups. • Gait is usually initiated by supraspinal influences and then maintained by CPGs. However, with appropriate sensory inputs gait can be initiated and maintained by CPGs. • Locomotor training was introduced in humans due to the success of training found in animal models.
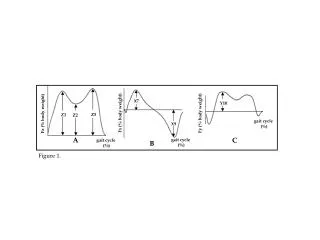
Sensory Cues Sensory Input essential to generation of normal gait pattern: • Maximum sustainable loading of the stance leg • Maintain an upright and extended trunk and head • Hip extension during terminal stance • Synchronous timing of hip extension with limb unloading and simultaneous loading of the contralateral limb (weight shift) • Maintain normal hip, knee, and ankle kinematics for walking • Avoid loading or weight bearing through the upper extremities • Minimize additional sensory stimulation that would conflict with the sensory information directly related to locomotion.
BWSTT Protocol • Treadmill speed - Gait velocity is selected based upon the clinical presentation of each patient and his/her ability to maintain balance and appropriate kinematics while at the same time promoting continuous stepping. - Generally, the ultimate goal is to achieve a normal walking speed (.75-1.25 m/s) • Amount of body weight support - 10%-40% of body weight support. The goal is to find the appropriate amount that will allow proper trunk and limb alignment and promote effective weight transfer onto bilateral lower extremities. • Ambulation kinematics - The goal is to maintain and promote all of the critical events of the normal gait cycle. This includes heel-strike, weight shift, controlled tibial advancement, and terminal hip extension during stance and knee flexion and dorsiflexion for toe clearance during swing.
BWSTT Protocol • Training Session Parameters - Ultimate goal of a training session is to achieve 20 minutes of gait. - Cycles of gait can be broken down into three minute bouts with standing rest periods in between. - Duration of sessions can be modified based on patient fatigue and ability to maintain joint kinematics and proper weight shift. • Progression to overground ambulation - Use of walkers, canes, etc. is avoided if possible because these devices can interfere with normal gait kinematics and promote upper extremity weight-bearing - However, certain patients may require an AD in order to maintain correct postural alignment or assist in balance. In this case, a long trekking pole and/or walking sticks can be used. - In addition, walkers may need to be modified in order to eliminate a forward flexed posture and upper extremity weight bearing.
Equipment • Treadmill -A treadmill with variable speed and inclination settings is needed • Harness -A harness is needed if the patient is unable to achieve adequate balance or cannot support full body weight during ambulation • Trainers - Depending upon the needs of the patient, up to four therapists may be needed to provide manual cues at the hip, knee, ankle, and upper extremity in order to facilitate normal gait kinematics • Mirror - Provides the patient with visual feedback for correction of proper body alignment
Manual Contacts • Hip - Therapist’s hands are located bilaterally on the posterior hip, overlying the superior portion of gluteus maxmius - External manual pressure is applied at the instant of initial contact in order to facilitate weight shift and single limb support • Knee - During the swing and stance phases of gait, the therapist can manually stimulate the hamstrings and quadriceps, respectively - In order to promote knee flexion, the therapist provides a quick pull on the medial hamstring tendon - For knee extension, the therapist applies a posterior force with his/her web space directly superior to the patella
Manual Contacts • Ankle -Therapist’s hand is located on the dorsum of the foot, directly inferior to the talocrural joint on the insertion of the tibialis anterior. - Toe clearance is achieved during the swing phase by lifting the foot and facilitating dorsiflexion • Upper Extremity - If assistance with arm swing is needed, the patient may grasp a pole in each hand as a therapist moves them in an anterior / posterior direction - Pole movement facilitates arm swing during gait
Patient Population • Spinal Cord Injury (SCI) -Patients with an ASIA classification of C or D have been shown to translate BWSTT to community ambulation and functional gains. These gains have been shown in those with both chronic and acute injury. - Patients with an ASIA A or B classification can still receive benefit from BWSTT such as cardiovascular conditioning, prevention of osteoporosis, prevention of ulcer sores, and prevention of metabolic diseases. These patients may not become fully ambulatory following intervention. • Cerebrovacascular Accident (CVA) - Patients who have suffered a stroke can also benefit from BWSTT. - Better walking and postural abilities were found in those who trained using body weight support than in patients who were gait trained bearing their full body weight. • Parkinson’s Disease (PD) - Initial studies indicate that BWSTT can improve the short-step gait pattern that is associated with PD. - Further studies are needed to evaluate the long-term effectiveness.
Efficacy Evidence • Spinal Cord Injury (SCI) - Several recent studies have demonstrated the effectiveness of BWSTT in the SCI population - Behrman, et al. have studied BWSTT extensively via case studies and have found that some persons have achieved higher FIM scores, greater gait velocity, decreased level of assistance, etc. • Cerebrovascular Accident (CVA) - Barbeau et. al. found that training gait in post-stroke patients using BWSTT resulted in better walking and postural abilities than gait training with full weight bearing. • Parkinson’s Disease (PD) - Miyai, et al. evaluated the use of BWSTT in treatment of patient’s with PD and found that while functional measures remained unchanged, gait speed and number of steps taken in 10 meters improved significantly - Further research has been indicated in order to investigate the role of BWSTT and delay of pharmocological intervention.
Other Considerations • Baclofen and other medications that are used to decrease muscle spasms may reduce the activity of the CPG by decreasing the sensory information available for processing in the spinal cord and by altering reflex activity. • BWSTT may lessen the amount of pharmacologic interventions that are needed to control spasticity by enabling appropriate activation patterns to be “learned”. • BWSTT allows patients to begin training as soon as they are medically stable, thus allowing intervention to begin earlier than with conventional gait training. • Everyone can potentially benefit for BWSTT due to its cardiovascular benefits. However, not all patients may progress to independent overground walking.
References • Barbeau, H. and Visintin, M. Optimal outcomes obtained with body-weight support combined with treadmill training in stroke subjects. Archives of Physical and Medical Rehabilitation. 2003; 84(October): 1458-1465. • Behrman, AL and Harkema, SJ. Locomotor training after spinal cord injury: A series of case studies. Physical Therapy. 2000; 80 (7):688-700. • Behrman, AL, Lawless-DIxon, AR, et. al. Locomotor training progression and outcomes after incomplete spinal cord injury. Physical Therapy. 2005;85 (12):1356-1371. • Behrman, AL, Bowden, MG and Nair, PM. Neuroplasticity after spinal cord injury and training: An emerging paradigm shift in rehabilitation and recovery. Physical Therapy. 2006;86 (10):1406-1424. • Miyai, I, Fujimoto, Y, et al. Long-term effect of body-weight-supported treadmill training in parkinson’s disease: A randomized controlled trial. Archive of Physical Medicine Rehabilitation. 2002;83:1370-1373