Download
1 / 12
120 likes | 169 Vues
Spinal Muscular Atrophy (SMA) is a neuromuscular disease characterized by motor neuron degeneration, muscle wasting, and weakness. Learn about SMA's genetic causes, clinical spectrum, symptoms, diagnosis methods, and comprehensive medical care, including genetic counseling. Molecular diagnostics techniques like MLPA are crucial for detecting mutations in the SMN gene. This condition requires a multidisciplinary approach involving various medical disciplines, therapies, and treatments. Discover more about SMA and its impact on individuals and families.

E N D
Spinal Muscular Atrophy BYMr.P.G.GEEGI, ASST.PROF, DEPT OF BIOCHEMISTRY, SJC, TRICHY. Course title: MOLECULAR DIAGNOSTICS (UNIT-I) CLASS: I M.Sc BIOCHEMISTRY.
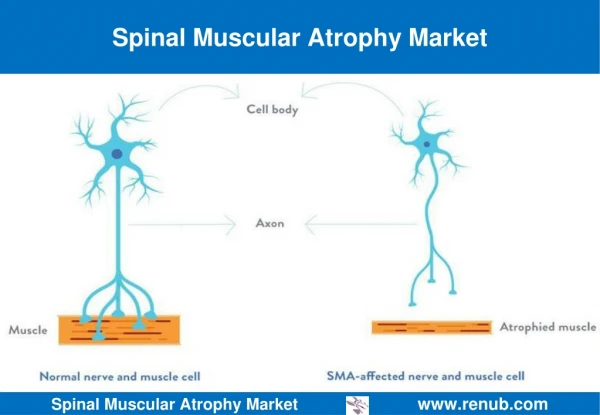
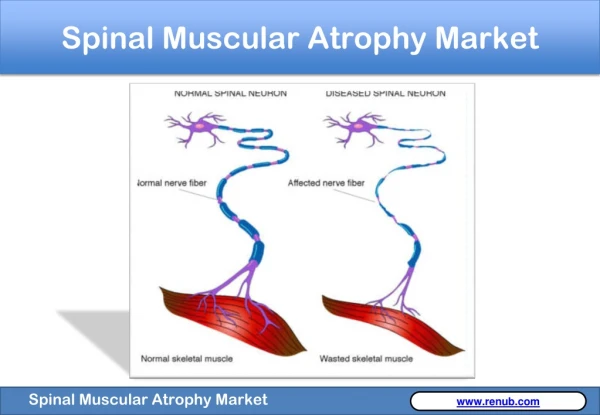
It is a neuromuscular disease characterized by degeneration of motor neurons resulting in progressive muscular atrophy (wasting away) and weakness. The clinical spectrum of SMA ranges from early infant death to normal adult life with only mild weakness. The most common form of SMA is caused by mutation of the SMN gene. The SMN gene is found on chromosome 5, the affected SMN gene is called SMN1. This gene involves breaking down and distributing protein, hence the muscle weakness as lack of protein causes muscle weakness and other problems .These patients often require comprehensive medical care involving multiple disciplinesincluding pediatric pulmonology,
pediatric neurology, pediatric orthopedic surgery, Lower Extremity & Spinal Orthosis, pediatric critical care, and physical medicine and rehabilitation; and physical therapy, occupational therapy, respiratory therapy, and clinical nutrition. Genetic counseling is also helpful for the parents and family members. Symptoms: The primary feature of SMA is muscle weakness, accompanied by atrophy of muscle contract. This is the result of denervation, or loss of the signal to that is transmitted from the spinal cord. This is normally transmitted from motor neurons in the spinal cord to muscle via the neuron's axon , but either the motor neuron with its axon, or the axon itself, is lost in all forms of SMA.
Many of the symptoms of SMA relate to secondary complications of muscle weakness, and as such can be at least partially remediated by prospective therapy. • muscle weakness • poor muscle tone • weak cry • weak cough • limpness or a tendency to flop • difficulty sucking or swallowing • accumulation of secretions in the lungs or throat • bell-shaped torso, caused by breathing using muscles around
the abdominal area • clenched fists with sweaty hands • flickering/vibrating of the tongue • head often tilted to one side, even when lying down • legs that tend to be weaker than the arms • legs lying in the "frogs leg" position • hypotonia, areflexia, and multiple congenital contractures (arthrogryposis) associated with loss of anterior horn cells • feeding difficulties • increased susceptibility to respiratory tract infections • bowel/bladder weakness.
lower-than-normal weight • developmental milestones, such as lifting the head or sitting up, can't be reached. Diagnosis: It can be made by the SMN gene test, which determines whether there is at least one copy of SMN1 gene by looking for its unique sequences in exons 7 and 8. In some cases, when the SMN gene test is not possible or does not show any abnormality, other tests such as an EMG electromyography (EMG) or muscle biopsy may be indicated. Genomic DNA was analyzed by MLPA, conventional PCR-RFLP, and allele-specific PCR .
Multiplex ligation-dependent probe amplification (MLPA) It is a variation of the PCR reaction that permits multiple targets to be amplified with only a single primer pair. Each probe consists of a two oligonucleotide which recognize adjacent target sites on the DNA. One probe oligonucleotide contains the sequence recognized by the forward primer, the other the sequence recognised by the reverse primer. Only when both probe oligonucleotides are hybridized to their respective targets, they can be ligated into a complete probe. The advantage of splitting the probe into two parts
is that only the ligated oligonucleotides, but not the unbound probe oligonucleotides, are amplified.If the probes were not split in this way, the primer sequences at either end would cause the probes to be amplified regardless of their hybridization to the template DNA, and the amplification product would not be dependent on the number of target sites present in the sample DNA. . Each complete probe has a unique length, so that its resulting amplicons can be separated and identified by (capillary) electrophoresis. This avoids the resolution limitations of multiplex PCR.
The forward primer used for probe amplification is fluorescently labeled, each amplicon generates a fluorescent peak which can be detected by a capillary sequencer. MLPA, is one of the only accurate, time-efficient techniques to detect genomic deletions and insertions (one or more entire exons), which are frequent causes of cancers such as hereditary non-polyposis colorectal cancer (HNPCC), breast, and ovarian cancer.MLPA can successfully and easily determine the relative copy number of all exons within a gene simultaneously with high sensitivity
REFERENCES • https://www.slideshare.net/suniu/immunodiffusion-principles-and-application. • https://ghr.nlm.nih.gov/condition/spinal-muscular-atrophy. • https://emedicine.medscape.com/article/1181436-overview.