Download
1 / 68
680 likes | 1k Vues
بسم الله الرحمن الرحيم. INTRAABDOMINAL HYPERTENTION & ABDOMINAL COMPARTMENT SYNDROME. important values. Normal intra-abdominal pressure is 0 - 5 mmHg. Pressures > 13 mmHg may be sufficient to restrict perfusion to the organs of the gut.

E N D
INTRAABDOMINAL HYPERTENTION & ABDOMINAL COMPARTMENT SYNDROME
important values • Normal intra-abdominal pressure is 0 - 5 mmHg. • Pressures > 13 mmHg may be sufficient to restrict perfusion to the organs of the gut. • If the abdominal compartment pressures is between 16-25 mmHg, hypervolemic volume expansion therapy can be used to maintain the perfusion pressure gradient for the abdominal organs. • When compartment pressures exceed 25 mmHg, decompression surgery should be considered to prevent organ damage. Pressure may rise rapidly with active bleeding. Edema (which occurs with any ischemic insult) will generally result in a later rise in the pressure (27 hours or more post insult).
Classify IAH into 4 groups: • Hyperacute(sec,min):laughing,strain,coug-hing,sneez,physical activities) • Acute(couple H):trauma,hge • Subacute (couple days): most medical cases. • Chronic: morbid obesity,intraabdominal tumor,pregnancy.
Patients at risk for ACS include: • trauma (blunt or open), as a result of the accumulation of blood, fluid or edema. • gastrointestinal hemorrhage can also lead to increased pressure in the abdominal compartment as ischemic cells swell or fluids collect. • pancreatitis • pneumoperitoneum • neoplasm
syndrome may follow a ruptured abdominal aortic aneurysm • intra-abdominal infection • Coagulopathies with abdominal bleeding • cirrhosis, or • profound hypothermia
massive intra-abdominal retroperitoneal hemorrhage, • severe gut edema • intestinal obstruction • ascites under pressure.
Patients who have undergone long surgical procedures with intraoperative hypotension and large fluid requirements are at significant risk, particularly if the abdomen has been closed under pressure in the OR. • External pressure from circumferential burns about the abdomen, application of military anti-shock trousers (MAST), or even tight abdominal restraint devices can cause tension within the abdomen due to external forces and result in ACS.2
Recently, awareness of the ACS has increased for 2 primary reasons. • First, the increased use of laparoscopy among general surgeons has brought with it an appreciation of IAP as a readily quantifiable entity. • Second, the more frequent use of planned repeat laparotomy for trauma has allowed both surgeon and intensivist to appreciate the beneficial effects of abdominal decompression upon removal of packing or evacuation of hematoma.
The Pathophysiology of IAH IAP VASCULAR COMPRESSION DIAPHRAGMATIC ELEVATION DIRECT ORGAN COMPRESSION RVP IVC Flow Cardiac compression Intrathoracic pressure Cardiac preload Cardiac contractility Systemic afterload PV pressure CARDIAC OUTPUT Renal Vascular Resistance Splanchnic Vascular Resistance RENAL FAILURE ABDOMINAL WALL ISCHAEMIA/OEDEMA RESPIRATORY FAILURE ICP SPLANCHNIC ISCHAEMIA
Compartment syndrome occurs when the pressure within a closed anatomic space increases to the point where vascular tissue is compromised with subsequent loss of tissue viability and function. This can occur within any closed body cavity.
Increased IAP leads to decreased MBF and to Bacterial translocation (BT),which may contribute to later septic complications and organ failure.
IAH provokes the release of pro-inflammatory cytokines which may serve as a second insult for the induction of MOF. • production of interleukin-1b (IL-1beta), interleukin-6 (IL-6), tumor necrosis factor (TNF-alpha)
Anaesthetic Implications ofACS: Pulmonary Implications Renal implications Porto-systemic visceral Implications Cardiovascular Implications Central nervous system Implications
Effects on CVS • As intraabdominal pressure increases above 10 mmHg, cardiac output declines, despite normal arterial pressures. • Additionally, whole body oxygen consumption, pH, and PO2 decrease. • Intraabdominal hypertension affects cardiac function by pushing the hemidiaphragms upward, thus transmitting the abdominal pressure to the heart and its vessels. • This decreases preload and increases afterload on the left ventricle and at the same time creates a hemodynamic picture of low cardiac output and high filling pressures.1,4
On the pulmonary system • The most commonly noted effects of IAH on the pulmonary system are elevated peak inspiratory pressures, decreases in Pao2 and increases in Paco2 requiring the use of complete ventilatory support to maintain adequate oxygenation and ventilation. • Hypercarbia, hypoxemia, and acidosis are evident when arterial blood gases are measured.6 • Positive end-expiratory pressure has been shown to exacerbate the cardiac and respiratory consequences of IAH.
Pulmonary effects of increased intra-abdominal pressure (2) • mechanical ventilation often necessary • high peak airway pressures ?barotrauma • high PEEP often required further compromising CO
Pulmonary effects of increased intra-abdominal pressure (3) Pressure on the IVC predisposes to venous stasis and increased risk of thromboembolism
Renal effects • include decreased renal plasma flow, glomerular filtration rate, and glucose reabsorption. Oliguria also occurs, with anuria noted in animal models when IAP reaches 30 mmHg.1 These effects occur without significant decreases in blood pressure(mechanical,↑ RVR,compression of R vein→outflow obstuction→↑ intraparenchymal pressure→shunting of blood from R cortex) . • Improvement of cardiac output does not improve renal function, nor do renal blood flow and glomerular filtration rate improve. • the placement of ureteral stents failed to improve renal function. • Improvement in renal function occurred only after abdominal decompression.7
These findings suggest that the effects of IAH on renal function are related to compression of the renal parenchyma itself and to compression of renal vasculature and are not related to decreased cardiac output. Other mechanisms proposed include shunting of blood away from the renal cortex into the medulla, decreased renal arterial flow with a concomitant increase in renal vascular resistance, and the presence of high levels of renin, aldosterone, and antidiuretic hormones.1
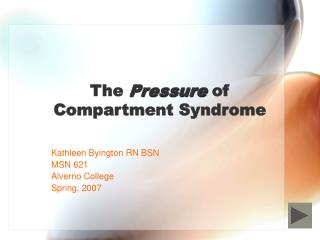
Experimental Control 20 Aldosterone level (ng/dl) 15 10 5 0 0 5 10 15 20 25 Fluids IAP (mmHg above baseline) Effect of increased intra-abdominal pressure on plasma aldosterone. The increased levels are reduced by volume expansion (J Trauma 1997;42:997-1003)
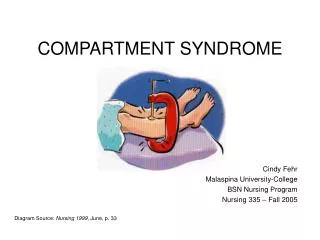
Plasma renin activity (ng/ml/hr) Experimental 30 Control 25 20 15 10 5 0 0 5 10 15 20 25 Fluids IAP (mmHg above baseline) Effect of increased intra-abdominal pressure on plasma renin activity. The increased levels are reduced by volume expansion (J Trauma 1997;42:997-1003)
IAH and Splanchnic Flow • Increases in IAP have adverse effect on splanchnic flow • >15mmHgSMA blood flow • marked reduction in hepatic artery and portal venous blood flow • leads to mucosal acidosis and oedema
Cycle of events created by IAH on splanchnic circulation Splanchnic hypoperfusion Hepatic ischaemia Gut mucosal acidosis Bowel oedema IAH Coagulopathy hypothermia acidosis Unrelieved ?Free oxygen radicals Distant organ damage Intra-abdominal bleeding ACS
They measured mucosal and intestinal blood flow and intramucosal pH (pHi) and found that mesenteric and mucosal blood flow decreased when IAP reached 20 mmHg, with intestinal mucosal flow declining to 61% of baseline. • At an IAP of 40 mmHg, intestinal flow decreased to 28% of baseline. • The intestinal mucosa showed signs of a severe degree of acidosis, measured by tonometer. These changes in splanchnic blood flow occurred despite maintenance of baseline cardiac output with volume loading.
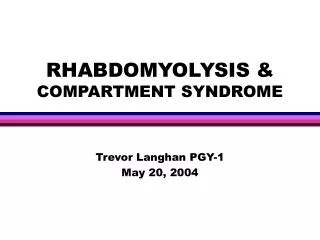
IAP 25mmHg for 60 min pp IAP 15mmHg for 60 min Baseline Bowel TPO2 5 3 Axillary TPO2 1 0 20 40 60 80 100 Effects of increasing IAP on bowel mucosal oxygen (tissue partial pressure, TPO2) compared with systemic tissue oxygenation in the axilla (J Trauma 1995;39:519-522)
blood flow to virtually every abdominal organ decreased significantly. The only exception was the adrenal gland; the reason this organ is not affected is unknown ?
EFFECTS ON CNS • The rise in intra-abdominal pressure, intrathoracic pressure leads to a rise in central venous pressure which prevents adequate venous drainage from the brain, leading to a rise in intracranial pressure and worsening of intracerebral oedema.
Intracranial Derangements and IAH • IAH associated with • ICP • CPP • cerebral ischaemia • ? Why? • may be due to impairment of cerebral venous outflow
increased intrathoracic pressure causing increased resistance to cerebral venous return associated with IAH( ?pseudotumor cerebri). • Volume expansion further increased ICP. Cerebral perfusion pressure declined as ICP increased and cardiac output declined. • Only abdominal decompression reversed effects of IAH. • The exact level of IAH that results in elevated ICP and decreased CPP in the brain injured patient is unknown;
Abdominal compartment pressure monitoring is done to help recognize life threatening elevations in pressure before ischemia or infarction of the abdominal organs occurs. When a patient exhibits a distended and taut abdomen, the measurement of abdominal compartment pressure can provide direction regarding the need for decompressive surgery.
Measurement of IAP Indirect Direct
Direct Monitoring • The most direct, accurate way to measure intraabdominal pressure is through an intraperitoneal catheter attached to a water manometer or pressure transducer, the preferred method in most experimental studies of IAH.1,6,15 Its use in the clinical situation is limited by the potential complications, specifically the risk of peritoneal contamination or bowel perforation. Abdominal pressure measured during laparoscopy is another example of direct measurement
Indirect Monitoring • Intraabdominal pressure may be indirectly measured by measuring pressure within certain abdominal organs. • The first indirect method described involves placement of transfemoral catheters into the inferior vena cava. The associated risks of this procedure include infection and thrombus formation. • measurement of gastric pressure through gastrostomy or nasogastric tubes • esophageal stethoscope catheter • urinarybladder pressure measurement.
Bladder Pressure Monitoring • At intravesical volumes less than 100 mL, the bladder acts as a passive reservoir, accurately reflecting intraabdominal pressure within a range of 5 to 70 mmHg.1,16 When bladder volumes exceed 100 mL, the intrinsic contraction of the bladder wall causes bladder pressure to increase.
The basic technique of bladder pressure measurement is not complicated. Fifty to 100 mL of sterile saline is injected into the bladder through a Foley catheter while the tubing to the drainage bag is clamped distal to the aspiration port. • The clamp is then opened to allow fluid to fill the tubing proximal to the clamp and the tubing is then reclamped. • A 16-gauge needle attached to a water manometer or a pressure transducer is then inserted into the aspiration port of the catheter, zeroed to the level of the symphysis pubis, and the intraabdominal pressure recorded. • Use of the pressure transducer attached to the bedside monitor allows a pressure waveform to be printed. Slight variation will be seen with the respiratory cycle. • Measurements should always be taken at end expiration because the diaphragm is elevated at this point, and thoracic pressure is less likely to influence the pressure reading
Patient positioning affects the accuracy of bladder pressure measurements. Monitoring should occur with the patient supine so that the weight of the abdominal contents pressing on the bladder does not falsely elevate the reading. Should the patient be unable to remain supine, the position at which the first measurement is taken should be noted and subsequent measurements taken with the patient in that position.2 Although the individual reading may be inaccurate, trends in abdominal pressure can still be assessed.
Others describe the use of a three-way Foley catheter, with the saline injected into one of the ports. Because three-way Foley catheters are not routinely used, their use requires either identification of the patient at risk before the catheter is inserted, or replacement with a three-way catheter when the need to measure IAP is identified. This increases costs and the potential for infection. Burch et al.7 described a technique in which the drainage tubing is clamped distal to the aspiration port and 50 mL of saline is injected through the aspiration port of the Foley catheter
Unfortunately, this procedure requires that the closed urinary drainage system be opened each time pressure is measured, placing the patient at increased risk of infection. • Strict aseptic technique is essential. A sterile towel should be placed under the Foley catheter to maintain sterility.
In patients having a neurogenic bladder or in those having a small contracted bladder (e.g., after radiotherapy), measurements may be inaccurate.
It is also possible that bladder pressure may not capture an elevation of the abdominal compartment pressure if there is a loculated area. • While abdominal compartment pressure monitoring via the bladder may provide valuable information regarding patients with abdominal hypertension, abdominal compartment syndrome should not be ruled out in the presence of a normal pressures if persistent clinical findings exist