Impact of Diabetes on Cardiovascular Health: Insights from Recent Studies
This summary highlights the interplay between type 2 diabetes and cardiovascular diseases (CVD), focusing on the acceleration of cardiac issues like left ventricular hypertrophy, diminished coronary reserve, and increased risk of myocardial infarction (MI) and heart failure (HF). It explores the 7-year incidence of fatal and nonfatal MI among diabetic vs. non-diabetic populations, revealing significant disparities. The role of hypertension and its management in reducing cardiovascular mortality rates in diabetic patients is also underscored, emphasizing the need for targeted interventions and monitoring.

Impact of Diabetes on Cardiovascular Health: Insights from Recent Studies
E N D
Presentation Transcript
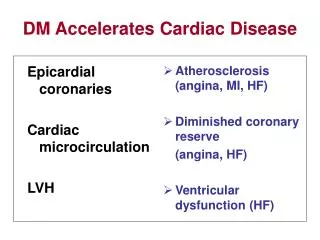
Epicardial coronaries Cardiac microcirculation LVH Atherosclerosis (angina, MI, HF) Diminished coronary reserve (angina, HF) Ventricular dysfunction (HF) DM Accelerates Cardiac Disease
Aorta and central arteries Arterioles Capillaries Arteriosclerosis and atherosclerosis (stroke, PAD, aneurysms) Hypertrophy and excess vasoconstriction (hypertension) Rarefaction Organ dysfunction (kidney failure, dementia, blindness) DM Accelerates Vascular Disease
Type 2 Diabetes and CHD: 7-Year Incidence of Fatal/Nonfatal MI (East-West Study) Non-diabetic N = 1373 Diabetic N = 1059 50 45 40 35 30 25 20 15 10 0 45% P<0.001 P<0.001 7-Year incidence of MI 20% 19% 4% No prior MI* MI No prior MI* MI MI=myocardial infarction. *These patients had no prior MI at baseline. Haffner SM, et al. N Engl J Med. 1998;339:229-234.
Systolic BP and CV Death Rates in Type 2 Diabetes 250 Nondiabetic Patients Diabetic Patients 200 Cardiovascular MortalityRate/10,000Person-yr 150 100 50 0 <120 120–139 140–159 160–179 180–199 ³200 Systolic Blood Pressure (mm Hg) Stamler J et al. Diabetes Care. 1993;16:434-444.
ALLHAT Biochemical Results: Fasting Glucose Chlorthalidone Amlodipine Lisinopril Total Baseline 123.5 (58.3) 123.1 (57.0) 122.9 (56.1) 4 Years 126.3 (55.6) 123.7 (52.0) 121.5 (51.3)* Among baseline non-diabetics with baseline <126 mg/dL Baseline 93.1 (11.7) 93.0 (11.4) 93.3 (11.8) 4 Years 104.4 (28.5) 103.1 (27.7) 100.5 (19.5)* Diabetes Incidence (follow-up fasting glucose 126 mg/dL) 4 Years 11.6% 9.8%* 8.1%* * In mg/dL, p<.05 compared to chlorthalidone
Risk of New-onset Diabetes Verdecchia, et al. Hypertension. 43:963-9, 2004
JNC 7 Medication Algorithm Initial Drug Choices Without Compelling Indications With Compelling Indications Stage 1 Hypertension(SBP 140–159 or DBP 90–99 mmHg)Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination Stage 2 Hypertension(SBP >160 or DBP >100 mmHg) 2-drug combination for most (usually thiazide-type diuretic and ACEI or ARB or BB or CCB) Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed Not at Goal BP Optimize dosages or add additional drugsuntil goal BP is achieved.Consider consultation with hypertension specialist.