Download
1 / 14
150 likes | 306 Vues
Data Integration Efforts and Challenges. Because Minds Matter: Collaborating to Strengthen Psychotropic Medication Management for Children and Youth in Foster Care August 27-28, 2012. Scott M. Bilder, Ph.D. Institute for Health, Health Care Policy, and Aging Research

E N D
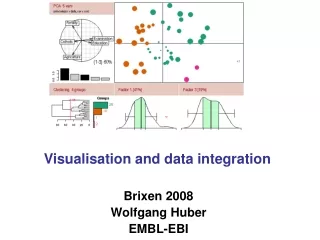
Data Integration Efforts and Challenges Because Minds Matter: Collaborating to Strengthen Psychotropic Medication Management for Children and Youth in Foster Care August 27-28, 2012 Scott M. Bilder, Ph.D. Institute for Health, Health Care Policy, and Aging Research Rutgers, The State University of New Jersey (bilder@rci.rutgers.edu)
MEDNET • AHRQ-funded initiative involving Rutgers, Columbia, Academy Health, six states, and othersto: • Develop a set of measures for antipsychotic use patterns. • Convene a cross-state network to review evidence, policies, and practices. • Implement quality improvement programs in each state. • Evaluate impact of efforts and share knowledge obtained.
MEDNET Organization • Multi-state Steering Committee / Learning Workgroup. • Workgroups (with representation from participating states). • Metrics Workgroup. • Foster Care Children Workgroup. • Duals/Medicare Part D Data Workgroup. • State-specific QI teams, including Project Leads, Data Leads, and Local Stakeholder Committees.
Adapting Efforts to Foster Care Context • Maintain existing relationships while developing new collaborations with child welfare stakeholders. • Broaden and diversify focus: • Shared (core) issues. • State-specific issues. • Identify appropriate data systems and experts. • Create and/or adapt quality metrics.
Data Issues • Identifying and tracking youth across time and data systems. • Keeping up with status/eligibility changes. • Identifying health services not captured in claims data. • Establishing sufficient look-back periods for treatment initiators. • Establishing common data structures to support analysis and reporting.
Data Sources Data Users Medicaid Encounter Data Medicaid Eligibility Files Data Integration Medicaid FFS Claims Medicare (A, B, D) Providersand Prescribers Mental Health Clinics State Childrens’ Services Data State Mental Health Agency Data Mental Health Carveouts Consumers DATA INTEGRATION State Mental Health Agencies State Children’s Services State Medicaid Agencies
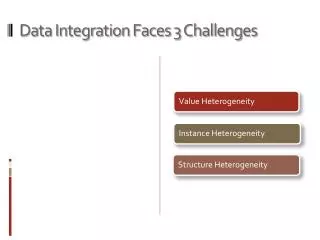
Data Integration • Multiple data silos are structured differently. • Often the data are structured to support very specific applications. • Narrative data present additional complications. • Data integration must happen at several levels: • Linkable databases. • Task-specific analytic files.
Data Integration • Full-scale integration of multiple data sources is often impractical given: • Different organization. • Different production schedules. • The sheer number of data elements. • We have found it useful to define a common data framework. • Using only those data elements that are needed. • Focusing programming efforts. • Focusing documentation efforts.
Privacy and Compliance • Different data sources present unique threats to privacy, and accompanying: • Request processes and agreements. • Person identifiers. • Physical security requirements. • Ongoing privacy review. • Data that we are used to handling in isolation may require additional efforts at privacy protection when combined.
Metric Development • Polypharmacy • Adherence • Excessive dose • Cardiometabolically challenging antipsychotics • Metabolic/lipid monitoring • Psychotropics in very young children • Diagnoses consistent with psychotropic treatment • Services consistent with psychotropic treatment
Metric Development • Metrics committee identifies needs with input from all stakeholders. • Initial discussions within metrics committee result in a draft conceptual summary. • Programming code is developed and results of applying metric are evaluated. • Conceptual summary is presented to stakeholder committee. • Metrics committee revisits evidence base on a regular basis.
Initiative Under Development • Develop partnerships to assist states in effectively utilizing systems for psychotropic medication monitoring and mental health quality improvement for foster care youth. • Facilitate knowledge sharing and integration. • Provide technical assistance.
Initiative Under Development • Develop, customize, and disseminate evidence on treatment effectiveness, processes, and quality management to states. • Monitor evidence base. • Create topic and technical briefs. • Provide participating states with customized products adapted to child welfare context. • Conduct webinars, panel discussions, to bring together multiple stakeholder perspectives.
Initiative Under Development • Improve the informatics foundation for bringing together multiple data sources. • Develop and/or adapt health care quality metrics to foster care context. • Identify and share best practices for linking data across and within state systems. • Develop a core multistate data model. • Implement a shared computing and documentation infrastructure. • Collaborate with states and others to design and conduct studies that make the most use of enhanced, linked databases.