Download
1 / 20

E N D
1. Carbon Monoxide and Cyanide Poisonings Working Version of Tutorial Presentation, Authors: MUDr. Petra Smolkov�,
Clinic of Occupational Medicine, Faculty Hospital and Palacky University Olomouc
2. Carbon Monoxide Poisoning, Occupational Exposure boiler-rooms, coceries, thermal powerstations
carbon monoxide
colourless odourless gas
product of incomplete combustion
3. Mechanisms of Toxicity toxicity
inhalation
200-300x higher binding capacity to hemoglobin than oxygen
development of carboxyhaemoglobinemia ? hypoxy, hypocapnia (=diminished oxygen-carrying capacity of the blood)
oxyhemoglobin dissociation curve (is shifted to the left) ? impairment of oxygen delivery to tissues
cytochrome oxidase ihibition
5. Clinical Symptoms immediate features
headache, nausea, irritability, weakness, tachypnoea
intermediate features
dizziness, ataxia, agitation, impairment of consciousness, respiratory failure
in seroius cases
cerebral oedema, metabolic acidosis
(less common) skin blisters, rhabdomyolysis, acute renal failure, pulmonary oedema, myocardial infarction, retinal haemorrhages, cortical blindness...
late features
neuropsychiatric features (after a few weeks), memory impairment, disorientation, apathy, inability to concentrate, personality changes, parkinsoninsm, incontinence ? very often total recover of symptoms within a year (or subtotal)
6. Indication of Severity acute neurological signs
coma
need for ventilation
ECG changes
acidosis
initial carboxyhaemoglobin > 30 %
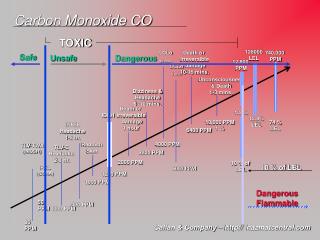
7. depends on the carboxyhaemoglobin level:
10% - light concentration impairment
20% - mild headache, vertigo
30% - headache, vomiting, dyspnea, fatigue
40-50% - persistent headaches, fuzziness, consciousness disorders, coma
> 60% - deep coma, death
8. Treatment removal from exposure
maintain a clear airway and ventilation
oxygenotherapy (oxygen in as high amount as possible)
transfer to hospital (serious states)
metabolic acidosis correction (by oxygenotherapy)
mannitol (if cerebral oedema is suspected)
ECG monitoring
measurement of carboxyhaemoglobin concentration
> 30 % - severe exposure
less than 30 % do not exclude significant poisoning!!!
look for extrapyramidal features and retinal haemorrhages to assess the severity of CNS damage (in pacients with unconsciousness in anamnesis)
controversial role of hyperbaric oxygen therapy...
10. Cyanide Poisoning, Professional Exposure hydrogen cyanide (HCN) and its gas, salts � potassium and sodium cyanide (KCN, NaCN);
nitriles (R-CN) � solvents, manufacture of plastics
industrial sources
metal and ore treatment, processing, printing, electroplanting, photoengraving, electronics, production of acrylics, plastics, nylon, petrochemical industry
fumigants, rhodenticides
acrylic nail remover and metal polishes!
combustion of polyurethane, rubber, nylon...
tobacco smoke!
drugs (sodium nitroprusside)
natural sources
cassava, some types of grasses, flax, lima beans, linseed
11. Mechanisms of Toxicity toxicity
soluble salts are more toxic (NaCN, KCN, CaCN)
ingestion of cyanide salts � hydrogen cyanide is producted by the contact with hydrochloric acid in stomach
gas inhalation
toxicity occures within a few seconds of HCN, death in minutes
ingestion of soluble cyanide salts
toxicity within minutes, absortion can cause toxicity for several hours
dermal exposure
large surface, onset may be delayed (several hours), epidermal necrosis
eye exposure
12. lethal dosis for hydrogen cyanide is 50 mg, sodium/potassium salts � 150 � 300 mg
cell breathing blockage (cytochromeoxidase), leads to metabolic acidosis, production od lactate, hypoxemia, venous blood is bright
detoxication (in the organism): ionic binding with sulphur (with thiosulphate sulofontranspherase) to almost nontoxic thiocyanate
13. Clinical Symtoms acute poisoning: cyanide, cyanogen chloride, acetonitrile, other cyanide releasing substances:
ingestion/inhalation, large amounts: cyanide concentration > 3 mg/l
immediate unconsciousness
convulsions
death in 1 � 15 minutes
ingestion/inhalation/ skin absorption, moderate amounts: cyanide concentration 1 � 3 mg/l
dizziness, tachypnoe, vomiting, flushing, headache, drowsiness, hypotension, rapid pulse, unconsciousness
death in convulsions in 4 hours (sodium nitroprusside � 12 hours)
ingestion/inhalation/skin absorption, small amounts: cyanide concentration < 1 mg/l
nausea, dizziness, drowsiness, hyperventilation, anxiety
14. acute poisoning: acrylonitrile, inhalation
nausea, vomiting, diarrhoea, weakness, headache, jaundice
absence of blood cyanide concentration � poisoning suggest:
lactate > 7 mmol/l, elevated anion gap acidosis, reduced arteriovenous oxygen gradient
16. Treatment based on the affinity of cyanide ion to methemoglobin - antidotes:
first aid
clear airway, ventilation
100 % oxygen to all victims
pulse, blood pressure, respiratory rate, oxygen saturation, cardiac rhythm monitoring
rapid transfer to hospital
17. mild poisoning
asymptomatic and mildly symptomatic patients
observation at least for 6 hours (ingestion of cyanide salt) or 12 hours (ingestion of acetonitrile)
natrium thiosulphate
18. moderate and severe poisoning
critical care
antidote therapy is necessary (if started in pre-hospital care the admitting hospital must be informed)
I. grade
immediately inhalation of amylium nitrosum (? methemoglobinemia cca 5 %)
hydroxycobalamine inj. 4 � 10 g i. v. or 4-DMAP inj. (3,25 mg/kg), causes methemoglobinemia 30 %
II. grade
natrium thiosulphate inj., 4 � 12 g i. v. (could be administred without additional antidotes in mild poisonings)
III. grade
only at a case of a definet cyanide poisoning can be administred cobalt EDTA (K�locyanor) � associated with severe allergic reactions
correction of hypotension (legs elevation, expanding the intravascular volume)
treatment of convulsions
19. Literature Fialov� J. Vybran� kapitoly z nemoc� z povol�n� II. Profesion�ln� intoxikace. Vydavatelstv� Univerzity Palack�ho, 2000. 51 p.
Pelclov� D et al. Nemoci z pov�ln� a intoxikace. Univerzita Karlova v Praze � Nakladatelstv� Karolinum; 2nd edition, 2006. 207 p.
Smedley J, Dick F, Sadhra S et al. Oxford Handbook of Occupational Health. Oxford University Press; 1st edition, 2007. 932 p.
20. Some cyanide, please... THANKS FOR YOUR ATTENTION!