Antimicrobial
Antimicrobial. General Information. -Medications used to treat bacterial infections. -Antibacterial is a natural, semi-synthetic or synthetic substance that kills or inhibits bacterial growth. Bacteriocidal – kills the bacteria Bacteriostatic – inhibit growth of bacteria

Antimicrobial
E N D
Presentation Transcript
General Information -Medications used to treat bacterial infections. -Antibacterial is a natural, semi-synthetic or synthetic substance that kills or inhibits bacterial growth. Bacteriocidal – kills the bacteria Bacteriostatic – inhibit growth of bacteria N.B.: Either after arresting the growth of the bacteria by a bacteriostatic or decreasing the number of viable bacteria by a bactericidal ,the body's immune system attacks, immobilizes, and eliminates the pathogens. If the drug is removed before the immune system has scavenged the organisms, enough viable organisms may remain to begin a second cycle of infection.
Antimicrobial drugs are effective in the treatment of infections because of their selective toxicity. (i.e): they have the ability to injure or kill an invading microorganism without harming the cells of the host. This term is is relative rather than absolute, requiring that the concentration of the drug be carefully controlled to attack the microorganism while still being tolerated by the host.
Factors Controlling Selection of the Antimicrobial Agent: 1) The organism's identity 2) The organism's susceptibility to a particular agent 3) The site of the infection 4) Patient factors 5) Safety of the Agent 6) The cost of therapy.
1-Identification of the infecting organism A-Gram staining A rapid assessment of the nature of the pathogen can sometimes be made on the basis of the Gram stain, which is particularly useful in identifying the presence as well identifying the morphologic features of microorganisms in body fluids that are normally sterile (CSF, pleural fluid, synovial fluid, peritoneal fluid, and urine). B-Culture it is essential to obtain a sample culture of the organism prior to initiating treatment. for definitive identification of the infecting organism to arrive at a conclusive diagnosis Sometimes , for definitive identification of the infecting organism ,other laboratory techniques, such as detection of microbial antigens, microbial DNA it or RNA, or detection of an inflammatory or host immune response to the microorganism is performed.
However, some critically ill patients require empiric therapy that is, immediate administration of drug(s) prior to bacterial identification and susceptibility testing. Ex. patient with severe headache, a rigid neck, and sensitivity to bright lights (symptoms characteristic of meningitis)”require immediate treatment. The choice of drug in the absence of susceptibility data is influenced by the site of infection and the patient's history (for example, whether the infection was hospital- or community-acquired, whether the patient is immuno-compromised, as well as the patient's travel record and age). Generally, broad-spectrum therapy are needed initially for serious infections when the identity of the organism is unknown
2-Determination of antimicrobial susceptibility of infective organisms After a pathogen is cultured, its susceptibility to specific antibiotics serves as a guide in proper choosing antimicrobial therapy. Even some pathogens, such as Streptococcus usually have predictable susceptibility patterns to certain antibiotics , others as gram-negative bacilli, enterococci, and staphylococcal species often show unpredictable susceptibility patterns to various antibiotics and require susceptibility testing to determine appropriate antimicrobial therapy.
3-Site of infection Adequate levels of an antibiotic must reach the site of infection for the invading microorganisms to be effectively eradicated. This is affected by : 1-Lipid solubility of the drug. 2- Molecular weight of the drug 3-Plasm Protein Binding.
4-Patient factors In selecting an antibiotic, attention must be paid to the condition of the patient. For example, the status of the patient's immune system, kidneys, liver, circulation, And age must be considered. In women, pregnancy or breastfeeding also selection of The antimicrobial agent Immune system: Elimination of infecting organisms from the body depends on an intact immune system. the host defense system must ultimately eliminate the invading organisms. Alcoholism, diabetes, infection with the human immunodeficiency virus, malnutrition, or advanced age can affect a patient's immunocompetence, as can therapy with immunosuppressive drugs. Higher-than-usual doses of bactericidal agents or longer courses of treatment are required to eliminate infective organisms in these individuals. Renal dysfunction: Poor kidney function (10 percent or less of normal) causes accumulation in the body of antibiotics that ordinarily are eliminated by this route. This may lead to serious adverse effects of drugs eliminated by the kidneys. Antibiotics that undergo extensive metabolism or are excreted via the biliary route may be favored in such patients.
Hepatic dysfunction: Antibiotics that are concentrated or eliminated by the liver (for example, erythromycin and tetracycline) are contraindicated intreating patients with liver disease. Age: Renal or hepatic elimination processes are often poorly developed in newborns, making neonates particularly vulnerable to the toxic effects of chloramphenicol and sulfonamides. Young children should not be treated with tetracyclines, which affect bone growth. Pregnancy: All antibiotics cross the placenta. Adverse effects to the fetus are rare, except the for tooth dysplasia and inhibition of bone growth encountered with the tetracyclines. Of course, all drugs should be used only during pregnancy under the supervision of a patient's physician. lactation: Drugs administered to a lactating mother may enter the nursing infant via the breast milk. Although the concentration of an antibiotic in breast milk is usually low, the total dose to the infant may be enough to cause problems.
5-Safety of the agent Many of the antibiotics, such as the penicillins, are among the least toxic of all drugs, because they interfere with a site unique to the growth of microorganisms. Other antimicrobial agents (for example, chloramphenicol) are reserved for life-threatening infections because of the drug's potential for serious toxicity to the patient. Note: safety is related not only to the inherent nature of the drug but also to patient factors that can predispose to toxicity
6-Cost of therapy Often, several drugs may show similar efficacy in treating an infection but vary widely in cost. It is more preferable to select suitable agent in its coast for treatment of certain infectious disease.
Ideal characteristics of antibiotics -selective toxicity with minimal side effects to host -easy to tolerate without a complex drug regimen -bactericidal rather than bacteriostatic -narrow spectrum rather than broad -low cost of production for consumer -stable (shelf-life) -adequate bioavailability: drug much reach adequate concentrations in relevant tissues or body sites A single agent is unlikely to meet all of these criteria
Combinations of Antimicrobial Drugs It is therapeutically advisable to treat patients with the single agent that is most specific for the infecting organism.This strategy reduces the possibility of superinfection, decreases the emergence of resistant organisms,and minimizes toxicity. However, situations in which combinations of drugs are employed do exist. For example, the treatment of tuberculosis benefits from drug combinations. Advantages of drug combinations Certain combinations of antibiotics, such as β-lactams and aminoglycosides, show synergism; that is, the combination is more effective than either of the drugs used separately. B. Disadvantages of drug combinations A number of antibiotics act only when organisms are multiplying. Thus, coadministration of an agent that causes bacteriostasis plus a second agent that is bactericidal may result in the first drug interfering with the action of the second. For example, bacteriostatic tetracycline drugs may interfere with the bactericidal effect of penicillins and cephalosporins
Mechanisms of Antibiotic Resistance Many species of bacteria have evolved resistance to certain antibiotics and synthetic agents - Resistance may develop if the target bacterial enzyme changes or if the bacteria evolves an alternate metabolic pathway - Bacteria may evolve the ability to enzymatically inactivate an antibiotic e.g. Β-lactamase - Bacteria may evolve the ability to prevent drug entry into the cytoplasm or to pump the drug out of the cytoplasm - Bacteria can evolve changes in drug targets like 30 S ribosomes binding site. Antibiotic Assays and Resistance
Complications of Antibiotic Therapy The drug may produce an allergic response or be toxic in ways unrelated to the drug's antimicrobial activity. A. Hypersensitivity Hypersensitivity reactions to antimicrobial drugs or their metabolic products frequently occur. For example, the penicillins, despite their almost absolute selective microbial toxicity, can cause serious hypersensitivity problems, ranging from urticaria (hives) to anaphylactic shock. B. Direct toxicity High serum levels of certain antibiotics may cause toxicity by directly affecting cellular processes in the host. For example, aminoglycosides can cause ototoxicity by interfering with membrane function in the hair cells of the organ of Corti.
C. Superinfections Drug therapy, particularly with broad-spectrum antimicrobials or combinations of agents, can lead to alterations of the normal microbial flora of the upper respiratory, intestinal, and genitourinary tracts, permitting the overgrowth of opportunistic organisms, especially fungi or resistant bacteria. These infections are often difficult to treat
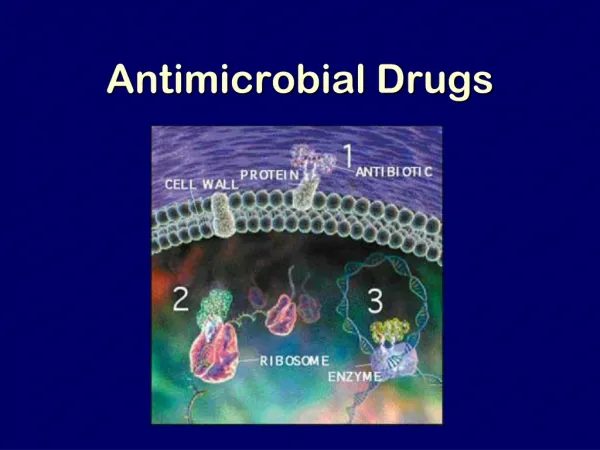
Mechanism of antimicrobial Agents 1. Inhibition of cell wall synthesis e.g. Penicillins, cephalosporins & vancomycin Human cells do not have a cell wall, so these drugs are specific only for bacteria. They will kill or stop replication of the bacteria without damaging the host. 2. Inhibition of protein synthesis e.g. Tetracycline, aminoglycosides, chloramphenicol, erythromycin Selective toxicity relies on the fact that the bacterial ribosome differs in size to the human ribosome
3. Inhibition of nucleic acid synthesis Affect microbial specific enzymes, e.g. DNA dependent RNA polymerase. 4. Antimetabolites Affect the metabolism of the organism by having a negative effect on some vital metabolite. Humans are unable to synthesize foliate and so must get it from the food, whereas bacteria must make their own. Hence, inhibition of foliate metabolism can hinder bacterial growth. e.g. Trimethoprim
Folate Antagonists Folate-derived cofactors are essential for the synthesis of purines and pyrimidines (precursors of RNA and DNA) and other compounds necessary for cellular growth and replication. Therefore, in the absence of folate, cells cannot grow or divide. To synthesize the critical folate derivative, tetrahydrofolic acid, humans must first obtain preformed folate in the form of folic acid as a vitamin from the diet. In contrast, many bacteria are impermeable to folic acid and other folates and, therefore, must rely on their ability to synthesize folate de novo. The sulfonamides (sulfa drugs) are a family of antibiotics that inhibit this de novo synthesis of folate.
Cont; Sulfonamides -One of the first groups of antibiotics -Bacteriostatic in action -Prevent synthesis of folic acid required for synthesis of purines and pyrimidines. -Does not affect human cells or certain bacteria that can use preformed folic acid -Examples: Short acting: sulfadiazine, sulfamethazine Intermediate acting : sulfamethoxazole Long acting : sulfathiazole , sulfasalazine
F. Spectrum of Activity -Broad range of Gm+ and Gm- -They are also active against some protozoa as toxoplasmosis and chloroquine-resistant malaria. G. Resistance - common due to: 1) an altered dihydropteroate synthetase. 2)decreased cellular permeability to sulfa drugs 3) enhanced production of the natural substrate, PABA.
H. Uses 1- Respiratory and urinary tract infection. 2-Ulcerative colitis 3-Skin wounds and skin burns. 4-Toxoplasmosis and malaria. 5-in burn units, creams of silver sulfadiazine or mafenide acetate have been effective in reducing burn-associated sepsis, because they prevent colonization of bacteria. However,Silver sulfadiazine is preferred, because mafenide produces pain on application. I. Side effects -Hypersensitivity reactions (e.g., rashes and drug fever) in a small number of patients. Other cause allergic reactions include photosensitivity. -Stevens-Johnson syndrome is also associated with sulfonamide use; it is characterized by fever, malaise, erythema ,and ulceration of the mucous membranes of the mouth and genitalia. -Hemolytic anemia may develop in persons with a genetic deficiency of red blood cell glucose-6-phosphate dehydrogenase (G6PD).
-High concentration of sulfonamides with aqueous solubility which is sufficiently low, the free drug or its metabolites may form crystals and cause bleeding or complete obstruction of the kidneys. i-Combinations of sulfa (for lowering the dosage of individual agents) ii- A lot of fluids intake iii-Alkalinization of the urine (to increase excretion) to reduce the chance of crystalluria -Sulfonamides compete for sites on plasma proteins that are responsible for the binding of bilirubin. As a result, less bilirubin is bound, and in the newborn, the unbound bilirubin can be deposited in the basal ganglia, causing kernicterus, a toxic encephalopathy. For this reason, sulfonamides should not be administered to newborns or to women during the last 2 months of pregnancy or lactating females. -Significant drug–drug interactions are those that potentiate the effects of other agents and require dosage reduction. These include certain anticoagulants, and hypoglycemic
D. Antibacterial spectrum -The antibacterial spectrum of trimethoprim is similar to that of sulfamethoxazole. It is active against most gram-positive and gram negative organisms. There is little activity against anaerobic bacteria.However, trimethoprim is 20-to 50-fold more potent than the sulfonamide.
E. Uses Trimethoprim may be used alone in the treatment of acute UTIs and in the treatment of bacterial prostatitis and vaginitis is used in the treatment of genitourinary, GI, and respiratory tract infections. F. Resistance Resistance in gram-negative bacteria is due to the presence of an altered dihydrofolate reductase that has a lower affinity for trimethoprim. Overproduction of the enzyme may also lead to resistance, because this can decrease drug permeability. G. Adverse effects Trimethoprim can produce the effects of folic acid deficiency.6 These effects include megaloblastic anemia, leukopenia, and granulocytopenia, especially in pregnant patients and those having very poor diets. These blood disorders can be reversed by the simultaneous administration of folinic acid, which does not enter bacteria.
III-Cotrimoxazole The combination of trimethoprim with sulfamethoxazole, called cotrimoxazole shows greater antimicrobial activity than equivalent quantities of either drug used alone .The combination was selected because of the similarity in the half-lives of the two drugs. Rationally, by blocking the first stepin folic acid synthesis, there is no real reason to block further steps. However, there are some bacteria which can inhibits the initial blockage, and so this may be the rationale for the use of such combination. -There is synergy between the two drugs - the combined effect is greater that the expected sum of their activities -Individually the drugs are bacteriostatic; however, in combination they are bactericidal -The use of two drugs will delay the emergence of resistance.
Mechanism of action • Resistance • -The bacteria by gentic mutation they do not need to make folic acid they utilize already formed folic acid. • -Overproduce the target e.g. To overcome trimethoprim, bacteria can overproduce DHFR to overcome the inhibition of trimethoprim. • -Bacteria produce mutated DHFR
Side effects TMP-SMX can cause the same adverse effects as those associated with sulfonamide administration. Most of the adverse effects of this combination are due to the sulfamethoxazole component. Uses TMP-SMX is used in the treatment of infection caused by ampicillin-resistant Shigella and for antibiotic-resistant Salmonella. -Successful in treatment of traveler’s diarrhea due to susceptible E. coli. -Because trimethoprim accumulates in the prostate, TMP-SMX is used to treat prostatitis caused by sensitive organisms. - Used n Pneumocystis jiroveci pneumonia occur in HIV patients.
Fluoroquinolones Fluoroquinolones were first introduced in 1986, they are modified quinolones, a class of antibiotics, whose accidental discovery occurred in the early 1960. The fluoroquinolones are a family of synthetic, broad-spectrum antibacterial agents with bactericidal activity. The parent of the group is nalidixic acid, discovered in 1962 by Lescher and colleagues. It was used orally for the treatment of infections caused by gram-negative organisms. The newer fluoroquinolones have a wider clinical use and a broader spectrum of antibacterial activity including gram-positive and gram-negative aerobic and anaerobic organisms
Mechanism of Action The fluoroquinolones enter the bacterium by passive diffusion through water-filled protein channels (porins) in the outer membrane. Once inside the cell, they inhibit the replication of bacterial DNA by interfering with the action of DNA gyrase (topoisomerase II) and topoisomerase IV during bacterial growth Binding of the quinolone to both the enzyme and the DNA forms a ternary complex that inhibits the resealing step, and can cause cell death. In gram-negative organisms ,the inhibition of DNA gyrase is more significant than that of topoisomerase IV, whereas in gram-positive organisms the opposite is true.
•Basis for Selective Toxicity - Quinolones have a relatively low affinity for mammalian DNA topoisomerase Mechanisms of bacterial resistance – change in target enzyme (DNA gyrase or topoisomerase IV) – change in permeability of organism (decrease in number of porin channles). -Increase in efflux of the AB.
Classification of Fluoroquinolones First Generation The first-generation agents include cinoxacin, pipdemic acid and nalidixic acid, which are the oldest and least often used quinolones. These drugs had poor systemic distribution , limited activity (against gram-negative bacteria not including psudomionas sp),and were used primarily simple urinary tract infections. - Cinoxacin and nalidixic acid require more frequent dosing (4 times daily) than the newer quinolones, and they are more susceptible to the development of bacterial resistance.
Second Generation. -The second-generation fluoroquinolones have increased gram-negative activity, as well as some gram-positive and atypical respiratory pathogen coverage. This is mainly due to inserion of F atom in position 6 in the naphthyridine core. -Compared with first-generation quinolones, these drugs have broader clinical applications in the treatment of :complicated urinary tract infections ,pyelonephritis, sexually transmitted diseases , and skin infections. -Agents of Second-generation include norfloxacin ,ciprofloxacin, enoxacin, lomefloxacin, and ofloxacin. -Ciprofloxacin and ofloxacin are the most widely used second-generation quinolones because of their availability in oral and intravenous formulations and their broad set of FDA-labeled indications.
N-cyclopropyle moity increased bioavilibility Ciprofloxacin
*Secound generation Fluoroquinolones advantages: -Active against gram-negative including Pseudomonas species and some gram- positive aerobic organism -Twice daily dosing. -Excellent oral absorption reached in some members to 99% -Excellent tissue penetration with prolonged half-lives -Overall safety
Third Generation. The third-generation fluoroquinolones are separated into a third class because of their expanded activity against gram-positive organisms (particularly penicillin-sensitive and penicillin-resistant S. pneumoniae) and atypical pathogens such as Mycoplasma pneumoniae and Chlamydia pneumoniae. -Although the third-generation agents retain broad gram-negative coverage, they are less active than ciprofloxacin against Pseudomonas species. -Because of their expanded antimicrobial spectrum, third-generation fluoroquinolones are useful in the treatment of community-acquired pneumonia -The third-generation fluoroquinolones include levofloxacin, gatifloxacin, moxifloxacin and gemifloxacin (maine adverse effect is rash in females under 40 years old).
Fourth Generation. The fourth-generation fluoroquinolones add significant antimicrobial activity against anaerobes while maintaining the gram-positive and gram-negative activity of the third-generation drugs. They also retain activity against Pseudomonas species comparable to that of ciprofloxacin. The fourth-generation fluoroquinolones include trovafloxacin (Trovan). -Because of concern about hepatotoxicity, trovafloxacin therapy should be reserved for life-threatening infections requiring in patient treatment (hospital or long-term care facility), and the drug should be taken for no longer than 14 days.