Aphasia
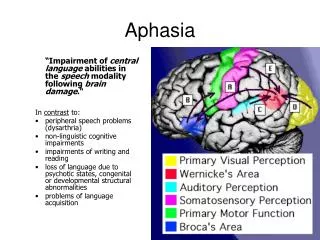
Aphasia. Def of Aphasia : A disorder of language that is neurogenic (caused by brain disease or injury), which involves the symbolic use of sound (i.e. Language in the meaningful sense of the word). Is not due to deafness or motor-paralysis, mental retardation etc. .

Aphasia
E N D
Presentation Transcript
Aphasia Def of Aphasia: A disorder of language that is neurogenic (caused by brain disease or injury), which involves the symbolic use of sound (i.e. Language in the meaningful sense of the word). Is not due to deafness or motor-paralysis, mental retardation etc.
Differential diagnosis and disorders which make it hard to identify aphasia • Dysathria – poor articulation of speech due to slurring or fragmentation of the sound structure of speech. Is a motor problem due to poor coordination of breathing and speech muscles. Cause slurred speech and staccato speech. • Apraxia – disorders of skilled movements. Can include symbolic movements. Cause by left parietal lesions. Some apraxias particularly affect the ability to speak, e.g Buco-facial apraxia.
Language is assessed in terms of: • Language comprehension: understanding language as opposed to hearing or seeing it • Language production: speech output, not just the utterance of noise, but the utterance of meaningful noise, and also the spontaneous production of language • Repetition: copying of language.
Other important terms • Anomia: ability to name things, tested on confrontation • Word-finding difficulties: difficulty finding the particular word you are looking for, seen in the patient’s spontaneous speech. • Paraphasia (next to speech) – distortions in speech output • Semantic paraphasias: say a word that is meaningfully related to the word you want to say. E.g. “whiskey” when you want to say “wine”. • Literal paraphasias: is phonologically different from the word you want to say. E.g. “broddel” instead of “bottle”.
Alexia –aphasia for written language (can’t comprehend) • Dyslexia – milder form of the above • Agraphia – disorder of writing, can’t produce (write) language. You can have an Alexia/agraphia without aphasia But you should not find an aphasia without an alexia/agraphia
Wernicke’s aphasia • Can’t comprehend, can’t repeat, can speak spontaneously • Spontaneous speech is however not normal • Is fluent, but is paraphasic, semantically paraphasic in particular. In extreme cases, word salad. • Make a particular type of literal paraphasic errors (neologism – make up new words, predominantly by putting old words together - Jargon aphasia. • Not always entirely aware that they are not making sense, because their comprehension is impaired. • Lesion site: left primary projection cortex (Wernicke’s area)
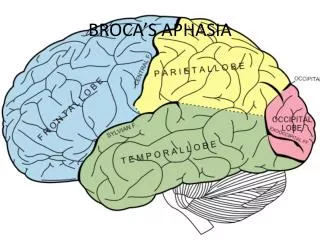
Broca’s aphasia • Speech out-put problems • Output is non-fluent, not only i.t.o. few words per minute (i.e. less than 60), but also in terms of short phrase length which leaves out connecting words and overemphasises of nouns. This leads to telegramatism. • Effortful and halting speech. • Lesion site: Just in front of motor area – Broca’s area: i.e. Posterior part of the inferior frontal convulsion • Same difficulties usually extend to written language
Conduction Aphasia • Comprehension and Production is still relatively intact • Repetition is impaired – sound images received by Wernicke’s area can not be transmitted forward to Broca’s area to be produced • However, spontaneous output is also not normal • Is paraphasic, but predominantly of literal type. This takes a particular form in that they will approximate the word closer and closer and sometimes they will get there • Lesion site: Posterior temporal lobe or insular cortex (track of fibres (white matter) that connects Broca’s & Wernicke’s area (arcuate fasciculus)
Transcortical sensory aphasia (TCSA) • Disruption to links between Wernicke’s area and the concept centre • Unable to comprehend, but still able to produce and to repeat • Circumlocutory – go around words. Leave out concrete words, but full of connectives • Speech is fluent, but empty of meaning • Severe word-finding difficulties, specifically for concrete words and nouns - Use phrases like “thing a ma jig” and “you know what” • Pathology: Alzheimer’s patients in the 2nd stage of disease. • Lesion: From Wernicke’s upwards towards parietal lobe.
Transcortical motor aphasia (TCMA) • Due to damage to fibres linking the concept centre with Broca’s area • Non-fluent speech output • Tend to say very little, lack of initiation of speech • Paucity of spontaneous output • Can repeat • Often has a compulsion to repeat back what is heard – echolalia • Lesion: Damage is to fibres that lead to Broca’s area. Is not always in transcortical area, lesion may also be in supplementary motor area.
Other types not included in Lichtheim’s model Global aphasia • Poor production and comprehension • Damage to both Wernicke’s and Broca’s area • Often a stroke may initially be cause a global aphasia and then recover to a Broca’s or Wernicke’s aphasia.
Mixed transcortical aphasia • Affect both transcortical motor and transcortical sensory fibres. • Caused by watershed infractions of middle cerebral area (thus speech area is isolated) • Can repeat, but can’t understand or produce. • Repeat quite a lot – echolalia
A cognitive neuropsychological framework for understanding language disorders Figure 3 shows a modular system or ‘functional architecture’ for identifying and producing spoken words
Acoustic/auditory analysis module: responsible for converting the speech signal of a word into a phonemic code • The Phonemic code can thenaccess that word’s entry in the auditory input lexicon • The auditory input lexicon is a store of information about the sound of each word that we know
The meaning of the activated word can become available within the semantic system • Semantic context can also aid word identification • Both the auditory input lexicon and the semantic system have links with the phonological output lexicon
The phonological output lexicon comprises of info about how to say all the words that we know. • Its output goes to a phonemic response buffer where the info about how to say the word is held until we are ready to say it. • There is also a two-way link between the phonological output lexicon and the phonemic response buffer - allows the two modules to become interactive in the generation of speech.
Thedirect link from the acoustic analysis system to the phonemic response buffer via the acoustic to phonological conversion system. Allows us to repeat nonsense words such as BLIG and SPONE. • Info can also flow from the phonemic response buffer back to the acoustic analysis module – this allows phonemic info to be recycled in the system and provides the basis for ‘inner speech’.
Disorders of Language (a psycholinguistic approach) Pure word deafness • This disorder provides evidence for the existence of a separable acoustic/auditory analysis module • Disorder is characterized by an inability to understand spoken words despite being able to read, write and speak normally
Can recognize music and environmental sounds, BUT has a specific problem in perceiving speech-like sounds. • The perceptual deficit responsible for pure word deafness involves a deficit in phonemic processing • I.e. the patient is unable to segment a string of speech sounds into its constituent phonemes
Pure word meaning deafness • Patient is unable to understand what a word means even though he/she is able to repeat and write words to dictation accurately • Auditory lexicon is intact – can distinguish between real words and non-words (i.e. still has a internal representation of each known word). • Semantic system is also intact, given that he/she is able to comprehend written material • Deficit lies in the connection between the auditory input lexicon and the semantic system.
Auditory phonological agnosia • This disorder provides neuropsychological support for the existence of a direct rout between the acoustic analysis module and the phonemic output buffer, i.e. that part of the system that allows us to repeat unfamiliar and non-words. • Patients loose the ability to translate acoustic inputs into speech – the only way in which we can repeat non-words. The only route for repetition becomes via the auditory input lexicon
Anomia • Is a condition in which the patient has problems finding the right word • Patients often resort to elaborate circumlocutions • E.g. for “doll” – they may say “solid representation of a baby” • Analysis of this disorder has been the primary basis for proposing an auditory output lexicon • Distinction between semantic anomia and word selection anomia
Semantic anomia: Patient has problems finding words because of a semantic disturbance – make semantic errors • In word selection anomia the semantic input appears intact (since these patients can understand what people are saying to them) and the defect lies within the phonological output lexicon itself.
Neologistic Jargonaphasia (Wernicke’s aphasia revisited) • These patients may suffer from a form of word selection anomia (which would explain the neologisms they make) • Is exacerbated by a failure to monitor the lexical status of words they produced – something termed ‘phonological derailment’ • It may be that attention may play a significant role in the fact that these patients are unable to monitor the errors they make when speaking