Download
1 / 15
160 likes | 300 Vues
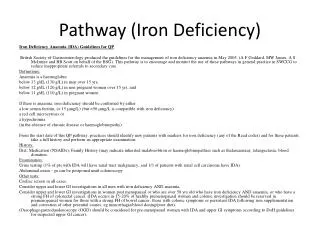
Iron Deficiency Anaemia -BSG guidelines 2011. Anaemia. Hb <13g/dL in men over 15 yrs Hb <12g/dL in non-pregnant women over 15yrs Hb <11g/dL in pregnant women over 15yrs Low MCV and MCH (ie microcytosis and hypochromia) are predictive factors of iron deficiency Other causes of the above.

E N D
Anaemia • Hb <13g/dL in men over 15 yrs • Hb <12g/dL in non-pregnant women over 15yrs • Hb <11g/dL in pregnant women over 15yrs • Low MCV and MCH (ie microcytosis and hypochromia) are predictive factors of iron deficiency • Other causes of the above
Investigations to define iron deficiency anaemia • Ferritin • 12-15 μg/l in patients with no inflammatory disease • 50 μg/l in patients with inflammatory disease • Iron studies: • Low iron level • Low transferrin saturation • Raised TIBC • Raised serum transferrin receptor
‘Functional’ iron deficiency anaemia • Chronic kidney disease • Inadequate iron supply to the bone marrow • Chronic diseases eg rheumatoid arthritis and IBD • Require iron supplementation prior to responding to erythropoetin
Causes • Contributor Prevalence • Occult GI blood loss • Common • Aspirin/NSAID use 10-15% • Colonic carcinoma 5-10% • Gastric carcinoma 5% • Benign gastric ulceration 5% • Angiodysplasia 5% • Uncommon • Oesophagitis 2-4% • Oesophageal carcinoma 1-2% • Gastric antral vascular ectasia 1-2% • Small bowel tumours 1-2% • Cameron ulcer in large hiatus hernia <1% • Ampullary carcinoma <1% • Ancylomasta duodenale <1%
Causes • Malabsorption • Common • Coeliac disease 4-6% • Gastrectomy <5% • Helicobacter pylori colonisation <5% • Uncommon • Gut resection <1% • Bacterial overgrowth <1% • Non-GI blood loss • Common • Menstruation 20-30% • Blood donation 5% • Uncommon • Haematuria 1% • Epistaxis <1%
History taking and examination • Family history • Haemoglobinopathies, colorectal cancer, angiodysplasias, bleeding disorders • Drug history eg NSAIDs, aspirin, steroids • Blood donation • DIET • Clinical signs eg. In Peutz-Jeghers or HHT
GI investigations • OGD • Gastric cancer or coeliac disease most definitive diagnoses to deter lower GI endoscopy • D2 biopsies plus TTG serology to diagnose coeliac disease • Colonoscopy vs radiology • Biopsy and removal of adenomata/polyps, viewing of angiodysplasias, NSAID damage • CT colonography detection rate of lesions >10mm: 90%
Coeliacs • Recommendations: • 1 year screening post diagnosis in patients >50yrs and with significant family history of colorectal carcinoma • Screening in patients with treated coeliac disease who develop IDA >50yrs old
Further investigations • Small bowel investigations • Capsule endoscopy • 40-50% diagnostic yield • Would have to perform invasive procedure to treat pathology • Small bowel enteroscopy • Many lesions detected reachable by gastroscope thus there is an end to repeating an OGD • Imaging eg MRI enteroclysis, ba meal & follow-through etc
Rarer causes • H.pylori infection • Decreases iron uptake and increases iron GI loss • Autoimmune gastritis • Giardia lamblia • Associated with diarrhoea • Small bowel (D2) biopsies & ELISA testing of stool • Angiogram • In transfusion-dependent anaemia
Treatment • Treat cause • Iron supplementation • Oral • Ferrous sulphate at 200mg bd or od for longer if poorly tolerated • Other preparations • Intravenous • Venofer, cosmofer • Ferric carboxymaltose (similar side effect profile but no anaphylaxis to date) • Transfusion
Follow-up • Once restored levels • 3 monthly first year • 1 year after that • Further investigations only if Hb and indices not maintained after above management • Most patients with negative upper and lower GI endoscopy and testing for coeliac disease, have no recurrence of iron deficiency
Special considerations • Pre-menopausal women • History for GI symptoms • Pregnant women • OGD, unsedated flexible sigmoidoscopy safe • MRI is advisable to avoid in the first trimester • Patients with significant co-morbidities • Patients due to have surgery • Transfusion than iron supplementation • Post gastrectomy patients • Iron loss also due to poor absorption of ascorbic acid • 2 to 3 fold increased risk of gastric cancer and increased risk of colorectal cancer • Post gastric banding iron deficiency responds to iron supplememntation
References • http://bsg.org.uk/images/stories/docs/clinical/guidelines/sbn/bsg_ida_2011.pdf