Diagnosis and Surgical Management of a Large Pelvic Mass: A Case Study
A patient presented to the ER with worsening chronic intermittent abdominal pain, nausea, and bloating. A CT scan revealed a large pelvic mass likely arising from the right adnexa, with multilocular characteristics and signs suggestive of a mucinous cystadenoma. Following exploratory laparotomy, total abdominal hysterectomy, right salpingo-oophorectomy, and mass removal were performed. The pathology confirmed the diagnosis. The case highlights the importance of careful evaluation of adnexal masses and the use of imaging in surgical planning.


Diagnosis and Surgical Management of a Large Pelvic Mass: A Case Study
E N D
Presentation Transcript
Pt. suffered from chronic intermittent abdominal pain for the last 3-4 months. Over the 24 hours prior to coming into the ER her pain is greatly worsened in severity. The pain radiates to her back and is accompanied by nausea and bloating. She has not had a bowel movement in three days, but has had flatus. She is afebrile. Pt. has a history of a partial bowel resection in 2004 for rectal prolapse. Abdomen is diffusely tender on physical exam. Her labs are negative, including HCG and CEA.
Supine AXR Upright AXR AXR shows bowel loops being displaced out of pelvis by a circular shaped 19 cm mass with soft tissue density. It appears to be distinct from the bladder wall.
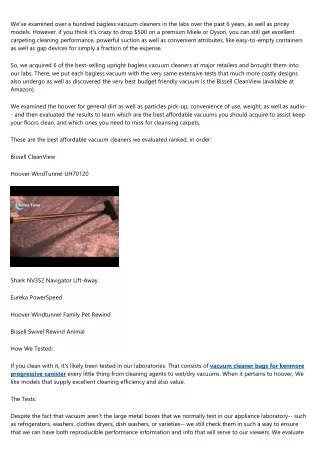
Transabdominal Ultrasound Axial Abdominal CT CT shows a large pelvic mass that appears to be arising from the right adnexa. Multilocular cyst with one primary cyst and some septations. US shows well-defined borders around hypoechoic space with acoustic enhancement posteriorly. There are septations and a mural nodule in the posterior wall. Mural does not show blood flow on Doppler but septations do. DePriest score of 8.
Adnexal Mass Differential • Cystadenoma (serous or mucinous) or cystadenocarcinoma • Hemorrhagic cyst (fenestrated without solid component) • Endometrioma (diffuse low level echoes) • Ectopic pregnancy • Teratoma (contains calcium and/or fat) • Abscess (air-fluid level) • Hematoma • Functional cyst (follicular, corpus luteum, or theca lutein) • Malignant lesions are more likely to have irregularities within the wall, thick septations, papillary projections, solid components, ascites, and size >9 cm. Blood flow within septations is a good marker of neoplasm, either benign or malignant. • DePriest score can be used to determine likelihood of malignancy. Its scoring system is based upon cystic wall structure, septation structure, and tumor volume. A score of 5 confers a higher likelihood of malignancy.
Hospital Course References Pelvic mass was not appreciated on AXR overnight, but was seen the following morning. A CT had already been order at the point due to the patient’s continued pain. The housestaff was notified of the mass, and the US was order for better characterization. A review of her February 2005 CT showed no mass at that time. She was admitted to the GYN service. She was taken to the OR after several days for exploratory laparotomy, TAH, RSO, removal of pelvic mass, and left oophoropexy. The frozen path was consistent with mucinous cystadenoma. She was discharged after about a week. Gay, Spencer and Woodcock, Richard. Radiology Recall. Lippincott, Williams, and Wilkins, 2000. pp. 582-584 Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging, 4th ed. Churchill, Livingston Inc., 2001. Pp. 2215-2218. Medical Student: Nicholas Nacey SMD ‘07