Download
1 / 26
300 likes | 376 Vues
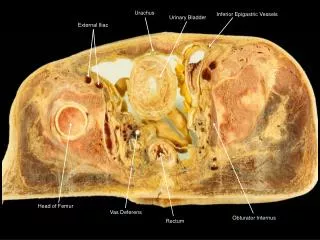
Treatment of iliac vein obstruction. George Geroulakos Professor of Vascular Surgery, University of Athens, Professor of Vascular Surgery, Imperial College, London. Surgical bypass for occluded iliac veins has now been largely replaced by endovenous stenting.

E N D
Treatment of iliac vein obstruction George Geroulakos Professor of Vascular Surgery, University of Athens, Professor of Vascular Surgery, Imperial College, London
Surgical bypass for occluded iliac veins has now been largely replaced by endovenous stenting.
Iliac/ IVC vein stenting is a recent development • Many of the endovenous techniques that are used are based on prior arterial experience
Morphologic and pathologic features of venous lesions are different from those of arterial stenosis. • Modification of standard techniques used in the management of arterial stenosis is necessary to obtain best results in endovascular interventions in the venous system.
Definitions • It is not known at what degree venous stenosis is haemodynamically significant • Morphological obstruction >50% as measured by IVUS has arbitrarily been chosen for stenting.
Systemic review of endovenous stenting in chronic venous disease secondary to iliac vein obstruction. • Conclusion: The quality of evidence to support this is weak, with the main flaw being the lack of control groups to illustrate the observed benefits are not part of natural history progression of CVD. Seager et al; Eur J VascEndovascSurg 2016
Stenting for total occlusions of the iliac vein • In a 9 year period 167 limbs in 159 post-thrombotic patients with total chronic occlusions of the iliac vein were treated. • Technical success: 83% • Cumulative pain relief at 3 years: 79% • Cumulative swelling relief at 3 years: 66% • Ulcer healing at 33 months: 56% • Raju, J VascSurg 2009
Venous stenting across inguinal ligament • Arterial stenting is not recommended across the inguinal ligament because of increased risk of focal neointimal hyperplasia or compression/fracture. • Venous stents can safely be placed across the inguinal ligament with no effect on log term patency.
Venous stenting across inguinal ligament 177 limbs had stents placed in the iliofemoral venous outflow across the inguinal ligament into the common femoral vein. Results compared with outcomes of 316 limbs with stents terminating above inguinal ligament. Cumulative patency was similar for both groups (7% versus 11% respectively) Neglen, J Vasc Surg 2008
Reflux & Obstruction Venous filling index VFI = 90VV / VFT90 Venous drainage index VDI = 90VDV/VDT90 mL/s
Venous drainage improves significantly after iliac stenting but this may result in faster venous filling Lattimer CR Kalodiki E Azzam M Schnatterbeck P Geroulakos G Josef Pflug Vascular Laboratory, Ealing Hospital & Imperial College http://josefpflugvascular.com No Disclosures
Aim To assess the hemodynamic impact of stenting in non-thrombotic iliac venous lesions (NIVLs)
Patients • 14 iliac veins in 10 patients stented • C0=1; C3=1 C4a=4; C4b=3; C5=3; C6=2 • 13 NIVL, 1 iliac occlusion • VFI & VDI pre/post stenting • CTV minor diameter (% stenosis) • IVUS: >50% area reduction = stent
RESULTS - clinical improvement • All legs improved (except 1 symptomless leg) • VCSS pre: 11 (7-12) post: 5 (4-8) p=.001 • Subjective • Softer in the ankle region • Lighter in colour in the ankle region • Lighter leg in weight/motion • Less swollen (10/14) - Lack quantitative measurements
Conclusion • The VDI is responsive to stenting in NIVLs • Clinical uses of the VDI may include - • Screening for obstruction • Assessment of CVI patients without reflux • Assessment of PTS patients with reflux • Selection for stenting • Monitoring stents