Download
1 / 22
220 likes | 1.35k Vues
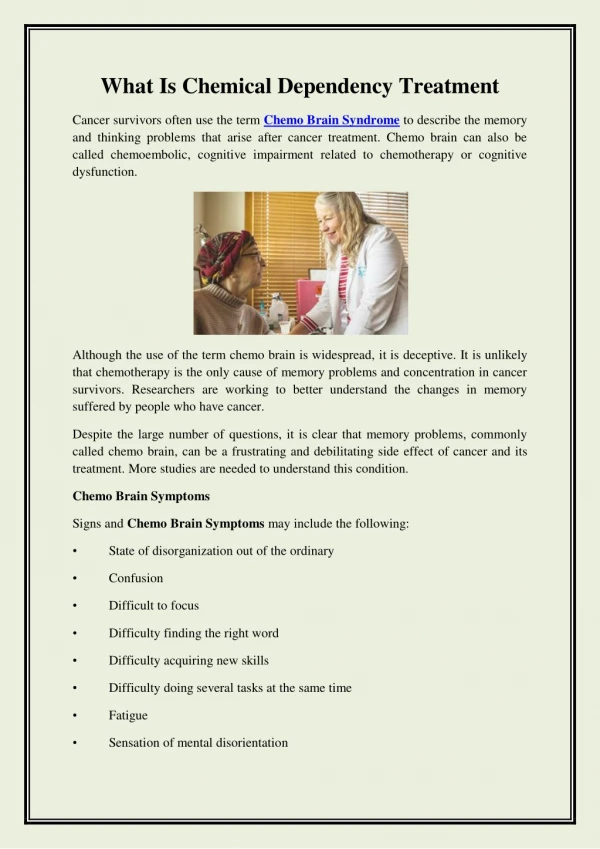
Chemical Dependency in Nursing. Sarah Casey Jeffery Hutchins Sumeka Rotasha Johnson Samjhana Joshi Wai Yee Law. Introduction . The terms “substance abuse” and “ chemical dependency” are often used interchangeably.

E N D
Chemical Dependency in Nursing • Sarah Casey • Jeffery Hutchins • SumekaRotasha Johnson • Samjhana Joshi • Wai Yee Law
Introduction • The terms “substance abuse” and “chemical dependency” are often used interchangeably. • “Substance Abuse” is associated with social factors, such as the failure to meet important obligations, multiple legal problems, drug-related arguments, and the use of drugs in dangerous situations. • “Chemical Dependency” is defined by physical factors, such as increased tolerance to drugs, withdrawal symptoms, an inability to control or decrease use, and continued use despite acknowledgement of the drugs’ dangerous effects.
The prevalence of substance abuse in general population averages 16 percent, the prevalence for nurses may be up to 20 percent. • This equates to approximately one in every 5 nurses who have substance abuse issues. • Substance abuse has been identified as an issue threatening the nursing profession since the turn of the last century.
History of Addiction among Nurses • During nineteenth century opiates, cocaine, and marijuana, were widely available, publicly advertised, unregulated, used as medicine before their addictive potential was known at the time. • During 1880, women outnumbered three to one to men in addiction. • Harrison Narcotic Act was passed in 1914 to control and regulate non-medicinal use of narcotics.
In 1920, the AMA Committee on the Narcotic Drug Situation, specifically mentions the overworked and over stressed nurse as being at “high risk for addiction”. • Due to the hidden nature of problem substance abuse in the nursing profession claimed little attention in the few nursing journals that existed at the time. • By the mid-1960s, narcotic addiction in nurses and physicians came to be considered a more serious problem than previously suspected.
Federal rehabilitation program designed specifically for addicted registered nurses began in 1972 at the Clinical Research Center in Lexington, Kentucky, but it was short lived. • Major help for nurses with addictive disease began in 1980 with National Nurses’ Society on Addictions when the society passed a resolution by acknowledging the problem and guidelines for impaired nurse programs.
Impact in Future of Nursing • “Best Nurse” is a label often given to impaired nurses who also often have graduated in the top of their classes, are perfectionists, highly motivated to be the “best”, the manager can count on to work overtime, come in on their day off, and to never say no. • With chemical dependency problem nursing has to loose such nurses especially during nursing shortage. • Nursing dependency needs to be addressed, and those already impacted need to be rehabilitated, not to lose the best nurse from the profession.
Significance on Profession of Nursing • Nurses with chemical dependency pose a threat to patient safety, their own health, and the reputation of the nursing profession. • In 1982, the American Nurses Association (ANA) first defined “impaired nursing practice” as the presence of dysfunction related to alcohol and other substance use or psychological problems that interfere with judgment and the delivery of safe care
Chemically dependent nurses jeopardize the standard of patient care as well as their own health. • Exposure to life-and-death situation, stress, long hours, difficult inter-professional relationships, workforce shortages and mandatory overtime increases the risk for these professionals to turn to substances as an unhealthy way to decompress. • Addressing this issue include assessment of late signs of addiction, appropriately confronted, and a holistic view of the causes and risk factors so that nurses can receive the intervention needed, achieve recovery and gain reentry into practice
Barriers to effectively address this issue: • Negative attitude • Discrimination both by colleagues and within insurance payment systems • Education of referring and intervening health professionals continuing punitive consequences to addicted nurses • Resource utilization and sharing • Research deficits • Workplace modifications that make drug diversion more difficult • Overall health promotion and prevention
Impact on 5 IOM Competencies • The 5 IOM Competencies are: • Provide patient-centered care • Work in interdisciplinary teams • Employ evidence-based practice • Apply quality improvement • Utilize informatics
To provide patient-centered care, nurses need to identify, respect, and care about patients’ differences, values, preferences, and expressed needs; listen to, clearly inform, communicate with, and educate patients; share decision making and management; and continuously advocate disease prevention, wellness, and promotion of healthy lifestyles, including a focus on population health. • To work in interdisciplinary team, they need to cooperate, collaborate, communicate, and integrate care in teams to ensure that care is continuous and reliable.
To apply evidence-based care nurses, need to integrate best research with clinical expertise and patient values for optimum care, and participate in learning and research activities to the extent feasible. • Applying quality improvement needs identifying error, providing safety, understand and measure quality of care, and design and test interventions to change process and system of care. • To utilize informatics, nurses need to communicate, manage knowledge, mitigate error, and support decision making using information technology.
Nurses under chemical influence often make errors in judgment and are involved on a number of incidents or mistakes. • Mood fluctuations, inappropriate responses or behaviors, confusion or memory lapses, isolation from colleagues and providing implausible excuses for behavior are a few of the social warning signs that a nurse with a chemical dependency may show. • These all affect the nurse to provide care based on the 5 competencies.
Legal and Ethical Issues • Most nurses with chemical dependency will not reach out for help because they are afraid of legal action. • According to the Technical Assistance Manual: Title I of the Americans with Disabilities Act; alcoholism is a disability, but drug addiction is not listed as a disability.
An individual pulling narcotics from workplace is open to disciplinary or legal actions such as the employer may deny or discharge employment. The employer will not be considered liable for disability discrimination. • There is a “Last chance agreement” to provide the individual with one more chance to change his/her current issues, where employee agree to frequent drug screenings, improvement, probation period, attend a detox program, and abide by all workplace rules and regulations. • Title I of the Americans with Disabilities Act also state that an employer may not discriminate against individuals who have successfully recovered from chemical dependency.
Impact on NC Nurses • According to the Nursing Practice Act obtained from NCBON, the board of nursing can deny licensure to a nurse, revoke the license of an RN, refuse to renew the license, and/or place the individual on probation. • A nurse’s scope of practice might also be temporarily or permanently limited, may be required to work in an office setting or on a unit with no access to narcotics. The time frame is usually from 6 months to a year after a chemical dependency recovery program has been completed.
Impact on Role of Nursing • Professional Practice • Increased risk of harming patient(s) • May lose respect & trust of colleagues • Loss of self respect • May be fired, suspended and/or placed on probation • Loss of income and seniority • May lose license • Will be monitored if allowed to return to practice
Why are Nurses at Risk? • Impaired nurses share some contributing and predisposing factors with the general population: • Chaotic family background • Low self esteem • History of victimization • Family history of substance abuse • Risk factors that relate to their profession: • They see evidence of the efficacy of drugs, also known as “pharmacological optimism.” • They have access to drugs. • They have a stressful workload and a demanding work environment.
Professional Responsibility: • As a licensed professional, your primary responsibility is the care and safety of patients. • You are legally and ethically required to report violations of your state’s nursing code and statutes that put patients at risk. • ANA suggests: Consult supervisory personnel; Follow organizational policies for documenting or reporting; If organizational policies are non-existent or inadequate, consult your professional association, state peer assistance program, employee assistance program or a similar resource.
References • American Psych, A. (2000). Diagnostic and statistical manual of mental disorders, dsm-iv-tr.. (4th ed. ed.). Arlington VA: American Psychiatric Publishing, Inc. • American Nurses Association. (1982). Position statement on impaired nursing practice. Kansas City, MO: Author. • American Nurses Association, the Center for Ethics and Human Rights. (2002). Code of Ethics for Nurses, with Interpretive Statements. Washington, DC: American Nurses Publishing. • Guidelines for Managers Working with Impaired Nurses: Nurses with Chemical Dependency and/or Psychiatric Issues. Ohio Nurses Foundation. Retrieved from http://www.ohnurses.org/Content/NavigationMenu/Resources/PeerAssistanceGuidelinesforManagersofImpairedNurses/Impaired_Nurses.pdf • Health Professions Education: A Bridge to Quality. Institute of Medicine, 2003. • Heise, B. (2003). The historical context of addiction in the nursing profession: 1850-1982. Journal of Addictions Nursing, 14(3), 117-124. • Lillibridge, J. (2010). Impaired nursing practice – what are the issues? In C. J. Huston (Ed.), Professional issues in nursing: Challenges & opportunities (2nd ed.) (pp. 275-286). Philadelphia, PA: Lippincott Williams & Wilkins.
Monroe, T., & Kenaga, H. (2011). Don’t ask don’t tell: Substance abuse and addiction among nurses. Journal Of Clinical Nursing, 20(3-4), 504-509. doi:10.1111/j.1365-2702.2010.03518.x • National Council of State Boards of Nursing (2007). Alternative programs. http://www.ncsbn.org. • National Council of State Boards of Nursing (NCSBN). (2011). Substance Use Disorder in Nursing: A resource manual and guidelines for alternative and disciplinary monitoring programs. Retrieved from https://www.ncsbn.org/SUDN_10.pdf. • Naegle, M. A. (2003). An overview of the American Nurses’ Association’s action on impaired practice with suggestions for future directions. Journal Of Addictions Nursing, 14(3), 145-147. doi:10.1080/10884600390245730 • Trinkoff, A. M., Eaton, W. W., & Anthony, J. C. (1991). The prevalence of substance abuse among registered nurses. Nursing Research, 40, 172-175. • Trinkoff, A. M., Shou, Q., & Storr, C. L. (1999). Estimation of the prevalence of substance use problems among nurses using capture-recapture methods. Journal of Drug Issues, 29, 187-198. • Wills, M. J. (n.d.). Is your nursing colleague impaired. Retrieved from http://tlcprojects.org/NEAT/ImpairedNurse_textversion.html