Download
1 / 38
380 likes | 548 Vues
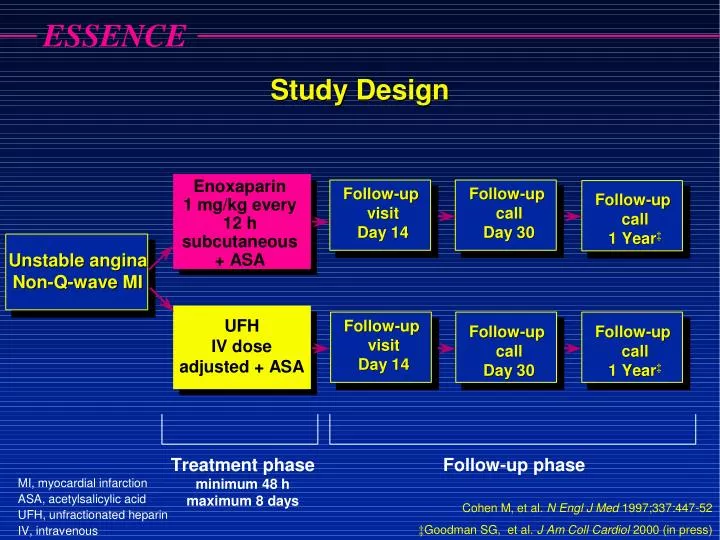
Major Hemorrhagic Events (Acute Phase) No significant increase in rate of major hemorrhage. 60. Number of patients. NS. UFH. Enoxaparin. 40. NS. NS. 20. 0. ESSENCE n = 3171. TIMI 11B n = 3910. TESSMA n = 7081. UFH, unfractionated heparin; NS, not significant.

E N D
Major Hemorrhagic Events (Acute Phase) No significant increase in rate of major hemorrhage 60 Number of patients NS UFH Enoxaparin 40 NS NS 20 0 ESSENCE n = 3171 TIMI 11B n = 3910 TESSMA n = 7081 UFH, unfractionated heparin; NS, not significant Antman EM et al. Circulation 1999;100:1602-8
Severe / moderate hemorrhage Death or re-MI Abciximab + 7.4% 4.6% reteplase D = 2.3% P < 0.001 D = 1.4% P = 0.001 8.8% Reteplase 2.3% 6 4 2 0 2 4 6 8 10 Percentage of patients GUSTO V Benefit vs. risk GUSTO V Investigators. Lancet. 2001;357:1905.
Low-Molecular-Weight Heparin Advantages Disadvantages • Increased anti-Xa to anti-IIa activity inhibits thrombin generation more effectively • Induces ↑ release of TFPI vs UFH • Not neutralized by platelet factor 4 • Less binding to plasma proteins (eg, acute-phase reactant proteins) more consistent anticoagulation • Lower rate of HIT vs UFH • Lower fibrinogen levels • Easy to administer (SC administration) • Long history of clinical studies and experience, FDA-approved indications • Monitoring typically unnecessary • Indirect thrombin inhibitor • Less reversible • Difficult to monitor(no aPTT or ACT) • Renally cleared • Long half-life • Risk of HIT Hirsh J, et al. Circulation. 2001;103:2994-3018. TFPI = tissue factor pathway inhibitor; UFH = unfractionated heparin; SC = subcutaneous; aPTT = activated partial thromboplastin time; ACT = activated coagulation time.
IIa C AT IIa S Hep UFH Direct antithrombin AT Xa LMWH
Heparin fails to effectively inhibit Clot-bound Thrombin
Bivalirudin inhibits Clot-Bound and Circulating Thrombin
Bivalirudin: Unique mechanism of action overcomes the limitation of Heparin
Bivalirudin Advantage Compared to Heparin/Enoxaparin with GP IIb/IIa inhibitors,Bivalirudin monotherapy significantly reduces major bleeding while providing similar ischemic protection, and improves net clinical outcome.
IIa C AT IIa S Hep UFH Direct antithrombin AT Xa AT Xa Pentasaccharide LMWH
Fondaparinux: ASynthetic Factor Xa Inhibitor Intrinsic pathway Extrinsic pathway Antithrombin Xa Xa AT AT AT Fondaparinux THROMBIN II IIa Fibrinogen Fibrin clot Adapted with permission from Turpie AGG et al. NEngl J Med. 2001;344:619.
IXa VIIIa Ca2+ PL Xa Va Ca2+ PL Key Steps in Coagulation Pathway Intrinsic pathway Intrinsic pathway Extrinsic pathway 1 Inhibition of one molecule of factor Xa can inhibit the generation of 50 molecules of thrombin2 X Xa 50 IIa II Fibrin Fibrinogen 1. Rosenberg RD, Aird WC. N Engl J Med 1999;340(20):1555–64. 2. Wessler S, Yin ET. Thrombo Diath Haemorrh 1974;32(1):71–8. Clot
Fondaparinux:A Synthetic Inhibitor of Factor Xa • Once daily administration • Rapid onset (Cmax/2=25 min) • Half life: 15-18 h. • Effects reversible with administration of activated Factor VII (Novoseven®) • No liver metabolism • Renal clearance • No protein binding (other than AT) • No reported cases of HIT • No dose adjustment necessary in elderly Herbert JM et al. Cardiovasc Drug Rev. 1997;15:1. van Boeckel CAA et al. Angew Chem, Int EdEngl. 1993;32:1671.
OASIS-6: Randomized, Double Blind 12,000 Patients with STEMI < 12 h of symptom onset Inclusion: ST 2 mm prec leads or 1 mm limb leads Exclusion: Contra-ind. for anticoagulant, INR>1.8, pregnancy, ICH<12 mo. Lytics (SK, TPA, TNK, RPA), Primary PCI or no reperfusion (eg. late) Stratification UFH not indicated UFH indicated Randomization Randomization Fondaparinux 2.5 mg Placebo Fondaparinux 2.5 mg UFH JAMA 2006;295:1519-30
Primary Efficacy OutcomeDeath/MI at 30 Days 0.12 UFH/Placebo 0.10 Fondaparinux 0.08 0.06 Cumulative Hazard HR 0.86 95% CI 0.77-0.96 P=0.008 0.04 0.02 0.0 0 3 6 9 12 15 18 21 24 27 30 Days The OASIS-6 Trial Group. JAMA 2006;295:1519-30
Death or MI 3 or 6 months 0.12 UFH/Placebo 0.10 Fondaparinux 0.08 0.06 Cumulative Hazard HR 0.88 95% CI 0.79-0.99 P=0.029 0.04 0.02 0.0 0 18 36 54 72 90 108 126 144 162 180 Days The OASIS-6 Trial Group. JAMA 2006;295:1519-30
Primary: Efficacy: Death, MI, refractory ischemia 9 day • Safety: Major bleeds • Risk benefit: Death, MI, refractory ischemia, major bleeds • Secondary: Above & each component (especially deaths) at 30 & 180 d • Hypothesis: First test non-inferiority, then test superiority
Death at 6 Months Enoxaparin 0.06 Fondaparinux 0.04 Cumulative Hazard HR 0.89 95% CI 0.79-0.99 p=0.037 0.02 0.0 0 20 40 60 80 100 120 140 160 180 Days
Death or MI: 6 Months Enoxaparin 0.12 0.10 Fondaparinux 0.08 Cumulative Hazard 0.06 HR 0.91 95% CI 0.84-0.99 p=0.036 0.04 0.02 0.0 0 20 40 60 80 100 120 140 160 180 Days
Major Bleeding: 6 Months 0.06 Enoxaparin 0.05 0.04 Fondaparinux 0.03 Cumulative Hazard HR 0.72 95% CI 0.63-0.82 p<<0.00001 0.02 0.01 0.0 0 20 40 60 80 100 120 140 160 180 Days
Death, MI, RI or MajorBleedingat 6 Months Enoxaparin 0.15 Fondaparinux 0.10 Cumulative Hazard HR 0.87 95% CI 0.81-0.93 p<<0.00001 0.05 0.0 0 20 40 60 80 100 120 140 160 180 Days
Fondaparinux Advantages Disadvantages • Difficult to monitor (no aPTT or ACT) • Long half-life • Catheter thrombosis during PCI • SC administration • Potential exists for outpatient management • Once-daily administration • Predictable anticoagulant response • Fixed dose • No antigenicity • Potentially no need for serologic parameters • Does not cross the placenta • HIT antibodies do not cross-react • Decreased bleeding complications vs UFH or LMWH Simoons ML, et al. J Am Coll Cardiol. 2004;43:2183-2190.Yusuf S, et al. N Engl J Med. 2066;354:1464-1476.