Download
1 / 44
440 likes | 664 Vues
Dennis C. Russo, Ph.D., ABPP Head, Behavioral Medicine Clinical Professor of Family Medicine and Psychology Department of Family Medicine Brody School of Medicine, East Carolina University Katherine Buck, M.S., LMFT Doctoral Student, Clinical Health Psychology

E N D
Dennis C. Russo, Ph.D., ABPP Head, Behavioral Medicine Clinical Professor of Family Medicine and Psychology Department of Family Medicine Brody School of Medicine, East Carolina University Katherine Buck, M.S., LMFT Doctoral Student, Clinical Health Psychology Department of Psychology East Carolina University Session #D5b October 6, 2012 White Coat, Blue Doctor Taking a look at OVER-activated Clinicians Collaborative Family Healthcare Association 14th Annual Conference October 4-6, 2012 Austin, Texas U.S.A.
Faculty Disclosure We have not had any relevant financial relationships during the past 12 months.
Objectives • Describe burnout, including its signs and symptoms in medical and behavioral health trainees • List the differences between stress and burnout, and how both impact providers • Identify methods for assessing and treating burnout in one’s own practice • Describe ways in which medical providers and behavioral health providers can work together to reduce/prevent burnout in providers and trainees
Learning Assessment A learning assessment will be conducted involving each participant taking a brief written self-evaluation instrument assessing burnout. At the conclusion of the session, these instruments will be scored and reviewed. Participants will engage in group discussion with focus on identifying strategies relevant to personal management of burnout and use of identified strategies in training curricula.
If you haven’t done so, take a moment to answer the questions on the form you were given when you entered the room. • Please use the scoring key on the form you completed. • No one will see your answers! • Turn the form over and set it aside…. We’ll get back to it in a bit. Personal Exercise
White Coat,Blue Doctor Taking a look at OVER-activated Clinicians
Burnout is a pathologic syndrome that results from “prolonged occupational stress” • It is not stress, depression, fatigue, etc • Is anybody safe? • Career Level? • Gender? • Age? • Culture? What is burnout?
Emotional exhaustion • Depersonalization • Low personal accomplishment What are the three elements of burnout? Maslach & Jackson (1981). Journal of Occupational Behavior, 2, 99–113
Weakened sense of control in the work setting • Time pressure, patient load, work hours, chaos! • Increased responsibility coupled with decreased resources • Limited collegial support • Toxic work culture • Emphasis on quantity over quality, lack of values • Additional risk factors for students! • New job, leaving family, stress on intimate relationships Risk factors for burnout Robinson, Gould, & Strosshal, (2010)
Maslach and Leiter (1997) – view burnout as gradual EROSION in three main areas: • Erosion of engagement: initial energy, involvement, and engagement of early practice are replaced by exhaustion, cynicism, and ineffectiveness • Emotional Erosion: initial enthusiasm, patience, and compassion of early practice are replaced by anger, cynicism, and bitterness • Erosion of fit: initial feelings of fit (career), and excitement of being part of medicine are replaced by lack of fit, discomfort, lack of belonging, and isolation How does Burnout Impact Health Professionals? Source:Wellness Book for Emergency Physicians, ACEM, 2004
Source: http://www.churchlink.com.au/churchlink/forum/r_croucher/stress_burnout.html
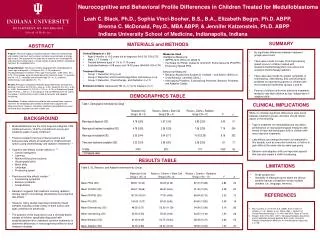
Burned-out residents are significantly more likely to self-report providing at least one type of suboptimal patient care at least monthly (53% vs. 21%; P = 0.004) • In multivariate analyses, burnout—but not sex, depression, or at-risk alcohol use—was strongly associated with self-report of one or more suboptimal patient care practices at least monthly (odds ratio, 8.3 [95% CI, 2.6 to 26.5]) Burnout has an impact on the patient too….Burnout and Self-Reported Patient Care Shanafelt, et al., Ann Intern Med March 5, 2002 136:358-367
Medical Errors and Burnout Shanafelt, et al., Ann Intern Med March 5, 2002 136:358-367
Increased risk of obstetrical complications for pregnant residents versus other working women1 • Premature labor is twice as common • Preeclampsia is twice as likely High rates of depression occur among residents 2 • 30% of first-year residents report depressive symptoms • Some reported to have suicidal ideation with plan Among married residents, 46% in depressed group versus 7% in the non-depressed group had marital problems (none of the depressed individuals had ever had martial problems prior to depression onset) • 1. Osborn LM, et al. J FamPract. 1990. • 2. Valko RJ, et al. Dis Nerv Syst. 1975. Sleep Deprivation and Resident Health – Contributor to or Outcome of Burnout?
Work Hours, Medical Errors, and Workplace Conflicts by Average Daily Hours of Sleep* *Baldwin and Daugherty, 1998-9 Survey of 3604 PGY1,2 Residents American Academy of Sleep Medicine
PubMed search on use of terms physician, burnout, and Maslach in studies between 1984 and 2001 • 46% to 80% report moderate to high levels of emotional exhaustion • 22% to 93% report moderate to high levels of depersonalization, • 16% to 79% report low to moderate levels of personal achievement Components of Burnout are Common among Practicing Physicians Chopra, JAMA. 2004;291(5):
Faculty surveyed in Internal Medicine Academic Dept. • 34% met criteria for burnout • Amount of time spent on activity that was most meaningful to faculty was strongly related to burnout • Faculty who spent less than 20% of time on activity most meaningful to them = more burnout • Optimizing career fit reduce burnout • Burnout and age only two variables associated with intention to leave academia Burnout in Academic Medical Faculty Shanafelt, et al., Arch Internal Medicine (2009)
Five hundred and seventy one doctoral psychologists in solo, independent group, or agency practices Emotional Exhaustion in Psychologists Rupert, P.A.& Morgan, D.J. Professional Psychology: Research and Practice 2005, Vol. 36, No. 5, 544–550
Solo and group independent practitioners reported a greater sense of personal accomplishment than agency respondents. • Women experienced higher levels of emotional exhaustion in agency settings than in either solo or group independent practice, whereas men experienced higher exhaustion in group independent practice. • Greater emotional exhaustion was associated with less control over work activities, working more hours, spending more time on administrative tasks and paperwork, seeing more managed care clients and fewer direct pay clients, and having to deal with more negative client behaviors. • Increased number of individuals with PTSD in a therapist’s caseload was found to be associated with increased burnout symptoms (Craig & Sprang, 2010) (as well as not using EBPs!) Work Setting and Burnout Among Professional Psychologists Rupert, P.A.& Morgan, D.J. Professional Psychology: Research and Practice 2005, Vol. 36, No. 5, 544–550
An International Study: US, UK, Canada, Germany, New Zealand, and Japan • Used MBI and found PA, DP, and EE predicted fair/poor quality of care • Increased work burden for nurses – reduced length of stay, etc. • High proportion of nurses with burnout across countries • Quality of care suffers (such as 30 day mortality) when nurses are burned out Burnout in Nurses Poghosyan, Clarke, Finlayson, & Aiken. (2010). Nurse burnout and quality of care: cross-national investigation in Six Countries. Research in Nursing & Health, 33, 288-298.
social workers with higher initial levels of burnout later reported more physical health complaints. • higher levels of burnout led to a faster rate of deterioration in physical health over a one-year period Burnout and Physical Health among Social Workers: A Three-Year Longitudinal Study of 406 Social Workers Kim Hansung, JiJuye, and Kao Dennis. Burnout and Physical Health among Social Workers: A Three-Year Longitudinal Study authored by Social Work Journal, Volume 53, Number 3, July 2011
MBI first published in 1981 by Maslach and Jackson (Journal of Occupational Behavior) • 22 item scale divided into 3 subscales • Emotional exhaustion • Depersonalization • Personal Accomplishment • 0-6 Likert Scale (0 = never, 6 = everyday) Maslach Burnout Inventory Maslach, C., Jackson, S. E., & Leiter, M. P. (1996). Maslach Burnout Inventory. (3rd ed.). Palo Alto, CA: Consulting Psychologists Press.
Assesses feelings of being overextended and exhausted by one’s work • High score = increased burnout Emotional Exhaustion
Measures an unfeeling and impersonal response toward recipients of one’s service, care, treatment, or instruction • High scores = increased burnout Depersonalization
Assesses feelings of competence and successful achievement in one’s work with people • Lower scores = increased burnout • *not correlated with the other two scales….. • PA is not the opposite of EE and Dp Personal Accomplishment*
Should not be labeled (BURNOUT inventory) • “MBI Human Services Survey” • Should not be administered by supervisors • Responsibilities of examiner = minimize response bias • Scales are calculated independently not one total score What should I know about using the MBI?
Advantages: • Relatively easy to give and score • Good measure of burnout construct (validity, test-retest) • Can be repeated over time • Disadvantages • No “healthy score” – large or small degree of burnout • No total cutoff score for burnout • Response bias issues in the workplace MBI – Advantages and Disadvantages Evaluating Stress: A Book of Resources http://www.rci.rutgers.edu/~sjacksox/PDF/EvaluatingStress.pdf
First degree: failure to keep up and gradual loss of reality • Second degree: accelerated physical and emotional deterioration • Third degree: major physical and psychological breakdown How Burned Out are You? Source: Physician Wellness & Burnout , Society for Academic Emergency Medicine
Based on empirically validated measure of experiential avoidance • Avoidance Getting “stuck” Frustration and burnout • Offers an estimate of the ability to use acceptance strategies during emotionally challenging moments • Personally meaningful action • Higher scores greater psychological flexibility PCP-AAQ Robinson, Gould, & Strossahl, (2010)
Provides information about specific sources of stress in the work setting • Covers 6 general areas (get a score between 0 and 1 for each) • Interactions with patients • Practice management • Administrative issues • Education and learning requirements • Relationships with colleagues • Balance between work and the rest of life • Can lead to PROBLEM FOCUSED COPING PCP-SC – a next step Robinson, Gould, & Strossahl, (2010)
Attitude/Behavior Changes: • Rapidly turns from compassionate and caring to abrupt, caustic • Withdraws from friends and activities • Becomes mistrusting, anxious, depressed, irritable Physical Changes: • Loss of appetite or reduced level of exercise • Looks tired; admits to insomnia • Personal hygiene deteriorates • Physical problems are self-treated Performance Changes: • Misses appointments • Make rounds at unusual hours • Can't be reached when on call • Sloppy charting • Smell of alcohol on breath during the day Relationship Changes: • Family communication deteriorates • Frequent arguments; spouse blamed • Occurrence of spouse, child abuse • Children may exhibit poor school performance • Jealousy, infidelity leading to separation, divorce Know the Warning Signs SOURCE: North Carolina Physicians Health Program - NCPHP
Personal • Influence happiness through personal values and choices • Spending time with family and friends • Religious or spiritual activity • Self-care (nutrition, exercise) • Adopting a healthy philosophical outlook • A supportive spouse or partner • Work • Control over environment workload • Finding meaning in work • Setting limits • Having a mentor • Having adequate administrative support systems Strategies to PreventPhysician Burnout Spickard, et al., JAMA. 2002;288(12):1447-1450 (doi:10.1001/jama.288.12.1447)
Residency is a powerful, formative experience in adulthood. • Establishing physician identity, schema of patient relationships, work habits, and self care. • Physician Burnout • Estimates of physician burnout: 25% - 70%. • Onset linked to residency training. • Distress in Residency • Dramatic increases in depression, anxiety, and drug use. • Increased cynicism, decreased empathy, poorer overall performance • Consequences • Psychological problems under diagnosed and under treated. • Physician stress and burnout linked to lower-quality patient care. • Habit of ignoring self care perpetuated in life after residency. The Importance of Early Teaching About Wellness & Well-being Source: Lebensohn, et. al., Resident Wellness and Well-being: Lessons Learned from the Integrative Medicine in Residency Program. PowerPoint Presentation from Arizona Center for Integrative Medicine.
Mindfulness Based Stress Reduction (MBSR) has been successful with decreasing stress at UMASS Medical School for over 20 years • Mindfulness – being “fully present” in the current moment • Burnout has been linked to depression as well as avoidant coping styles • Teaching alternative coping styles • Change the culture of training which engenders self sacrificing attitudes Adding Wellness to Training Programs Dobkin & Hutchinson, Medical Education, 2010
Kumagi, et al (2008) found that faculty physicians who facilitate small groups focused on psychosocial issues in patient care were more focused on humanistic aspects of their own patient care • Increased connection with other faculty and students • Increased reflection and skill development in their own practice • Source of personal fulfillment and renewal • Empathy can also be fostered in students by allowing time for reflection on critical events (Rosenthal, et al., 2011) Teaching – Focus on HumanismWatch one, do one, teach one?
An RCT with nurses (Turkey) showed decreased emotional exhaustion after an intervention targeted at coping and emotional support (Gunusen & Usten, 2010). • BUT, decreases in EE were not maintained at 6 mos • Suggests the need for continual intervention (support groups, etc), rather than a “one shot” deal • Skill-specific interventions (ACT, CBT) ? • Specific interventions for new trainees • Teach skills in school • Monitoring for “bullying” of new graduate nurses (offer career ladders, establish “hot-lines”, provide recognition of achievement, build networking in units) as bullying is related to burnout in new nurses (Laschinger, Grau, Finegan, & Wilk, 2010). Lessons from the nursing literature
According to Rosenberg & Pace (2006), MFTs (and other therapists!) can benefit from: • Openly expressing feelings about jobs and burnout • Taking regular vacations • Exercise/Proper diet • Setting limits for work/life balance • Psychotherapy (as clients) • Organizational level interventions: in-service training, decreased paperwork, shortening workdays, increasing workday breaks, and improved relationship between staff members What can therapists do?
Effective clinical supervision is related to lower levels of burnout in community nurses (Edwards, et al., 2006) • Lower levels of trauma-specific training predicted higher burnout and compassion fatigue in therapists working with traumatized patients (Craig & Sprang, 2010). • MFTs (especially those new to the field) may experience a buffer effect of clinical supervision and decreasing burnout (Rosenburg & Pace, 2006). Supervision, Supervision, Supervision!
Burnout in medical students and residents is prevalent • Don’t forget burnout in behavioral health professionals too! • Career satisfaction is directly related to burnout • Important to assess burnout AND mental health • Once you assess, take action! • Recommended reading: • Real Behavior Change in Primary Care (Robinson, Gould, & Strossahl, 2010) Take home points