Download
1 / 51
630 likes | 1.03k Vues
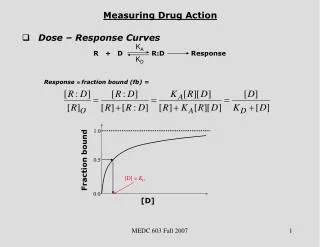
ELEVEN INTERNATIONAL SYMPOSIUM HEART FAILURE & Co Caserta, 29 – 30 aprile 2011. RANOLAZINE A NEW DRUG WITH A CLASS ACTION The anti heart failure action Pasquale Perrone Filardi Università Federico II di Napoli. Oxygen free radicals. Pathological conditions with increased I NaL.

E N D
ELEVEN INTERNATIONAL SYMPOSIUM HEART FAILURE & Co Caserta, 29 – 30 aprile 2011 RANOLAZINE A NEW DRUG WITH A CLASS ACTION The anti heartfailureaction Pasquale PerroneFilardi Università Federico II di Napoli
Oxygen free radicals PathologicalconditionswithincreasedINaL Zaza et al Pharm &Ther 2008 Heart failure Post-MI remodeling Ischemia
Positive feedback during ischaemia increases the imbalance between myocardial O2 supply and demand Ischemia O2 supply/ MVO2 X • extravascular compression ( O2 supply) Late INa Deleterious Positive Feedback Cycle Contracture ( LVEDP) [Na+]i NCX Ca2+ overload Arrhythmias
Electrical dysfunction Arrhythmias Mechanical dysfunction ↑Diastolic tension O2 supply & demand ↑ATP consumption ↓ATP formation Ranolazine: mechanism of action Ischaemia ↑ Late INa Ranolazine Na+ overload NCX Ca++ overload NCX: sodium-calcium exchanger Hasenfuss G, Maier LS. Clin Res Cardiol 2008;97:222-26. Maier LS. Cardiol Clin 2008;26:603-14. 4
Late INa is increased in failing myocytesLeading to QT prolonagtion, EADs and beat-to-beat variation in APD canine human Valdivia ,Journal of Molecular and Cellular Cardiology 38 (2005) 475–483 Maltsev et al. Eur J Heart Fail 2007
Time Course of Changes in LV End - diastolic Pressure (EDP) During Low Flow Ischemia B) Time to onset of contracture C) Average EDP (30min period) * 30 30 20 * Time (min) 20 10 EDP (mmHg) 10 0 Control RAN 0 Control RAN A)Time – dependent changes in EDP Control 70 Control 60 Contracture ( LVEDP) MVO2 O2 - Supply Ranolazine (10µM) 50 40 EDP (mmHg) Ranolazine 30 20 10 0 0 10 20 30 Time (min) Wang, JPET 321:213-220, 2007.
EFFECTS OF RANOLAZINE ON STUNNING MYOCARDIUM IN ISCHEMIA REPERFUSION INJURY 35,000 25,000 RPP (mmHg/min) 15,000 Control (10 µM) Ranolazine 5,000 0 10 20 30 40 50 60 Time (min) Hwang, JPET 321:213-220, 2007.
RANOLAZINE ATTENUATES THE INCREASE OF END-DIASTOLIC PRESSURE DUE TO PALMITOYL-L-CARNITINE –INDUCED INCREASE OF LATE INA Wu Y et al. J PharmacolExpTher 2009;330:550-7.
RANOLAZINE ATTENUATES THE INCREASE OF VENTRICULAR STIFFNESS DUE TO PALMITOYL-L-CARNITINE –INDUCED INCREASE OF LATE INA Wu Y et al. J PharmacolExpTher 2009;330:550-7.
EFFECTS OF RANOLAZINE ON lvend-diastolicpressurePOST CARDIOPLEGIA IN LANGENDORFF PERFUSED ISOLATED HEARTS Hwang H et al. Circulation. 2009;120 suppl 1:S16–S21
RANOLAZINE IMPROVES MECHANICAL EFFICIENCY IN A CANINE MODEL OF CHRONIC HEART FAILURE Chandler MP et al. Circ. Res. 2002;91;278-280
RastogiS et al. AmJPhysiolHeart CircPhysiol2008; 295: H2149–H2155
RastogiS et al. AmJPhysiolHeart CircPhysiol2008; 295: H2149–H2155
Ranolazine reduces the increase in diastolic tension in LV trabeculae from human failing heart Sossalla S et al. J Mol Cell Cardiol 2008; 45: 32-43.
EFFECTS OF RANOLAZINE ON FORCE AMPLITUDE AND DIASTOLIC FORCE ON ATRIAL MYOCITES FROM ATRIAL FIBRILLATION AND SYNUS RYTHM PATIENTS SossallaS et al. J Am CollCardiol 2010;55: 2330–42
EFFECTS OF VERAPAMIL ON DIASTOLIC FUNCTION IN RELATION TO AGE IN NORMAL INDIVIDUALS Arrighi,J, Perrone-Filardi P, et al. Circulation 1994; 90: 213-219
EFFECTS OF DILTIAZEM ON DIASTOLIC FUNCTION IN CAD PATIENTS Betocchi S, PerroneFilardi P, et al. AmJCardiol 1996;78:451-457
Ranolazine shortened a prolonged QTc interval and improved diastolic relaxation in patients with the LQT3-ΔKPQ mutation, a gentic disorder that is known to cause an increase of late sodium current
Effects of ranolazine on diastolic function in 22 patients with chronic angina Figuredoet al. J CardiovascPharmacolTher. 2010 Oct 5. [Epubahead of print]
Ranolazinesignificantlyreduced the primary end pointamong the high-riskcohortofpatientswith BNP>80 pg/ml in the MERLIN trial 21% (RRR) P=0,009
Ranolazine significantly reduced the primary end point among the high-risk cohort of patients with BNP>80 pg/ml
CONCLUSIONS AND PERSPECTIVES • Late INA is increased in diastolic and systolic heart failure • Ranoolazine reduces late INA and improves diastolic function in experimental animal models and in ex vivo human myocardium • Ranolazine also reduces post-ischemic contractile dysfunction • In vivo human data are so far scarce yet encouraging and shall be considered as proof of concept • Clinical studies are warranted to assess the effects of ranolazine on heart failure with preserved EF and on reperfusion (ACS) patients
Global left ventricular function, as assessed by the myocardial performance index, was significantly improved on drug therapy (p < 0.0001)
Late INa is involved in the Long QTS Normal Enhanced (KPQ) 5 pA 50ms 50 ms INaL INaL
L'aumento di INaL rallenta il rilassamento Phasic Phasic Tonic Twitch Abnormal Normal 0 0 Ao SodiumCurrent Late I Na Late INa P (mmHg) LV Peak Peak 1 2 (Plateau) 3 0 (Upstroke) 4 coronary flow (ml/min) Belardinelli, L. 2007
RastogiS et al. AmJPhysiolHeart CircPhysiol2008; 295: H2149–H2155
RastogiS et al. AmJPhysiolHeart CircPhysiol2008; 295: H2149–H2155
RastogiS et al. AmJPhysiolHeart CircPhysiol2008; 295: H2149–H2155
SossallaS et al. Journal of Molecular and Cellular Cardiology2008; 45:32–43
SossallaS et al. Journal of Molecular and Cellular Cardiology2008; 45:32–43
SossallaS et al. Journal of Molecular and Cellular Cardiology2008; 45:32–43