Download
1 / 13
130 likes | 257 Vues
Acute Medicine M5 Seminar (Hypoglycaemia). Yeo Xinying 19 Jan 2005. History. 75 yr old female Drowsiness for 1/7 Fever and vomiting for 2/7 Type 2 DM,20 yrs on glibenclamide 5 mg om. Examination. Drowsy Dehydrated BP 100/60 mmHg PR 100/min No other abnormal physical signs.

E N D
Acute Medicine M5 Seminar(Hypoglycaemia) Yeo Xinying 19 Jan 2005
History • 75 yr old female • Drowsiness for 1/7 • Fever and vomiting for 2/7 • Type 2 DM,20 yrs on glibenclamide 5 mg om
Examination • Drowsy • Dehydrated • BP 100/60 mmHg • PR 100/min • No other abnormal physical signs
Investigations 1)RP#2 - Urea 22.4 mmol/L (2.5-7.5) Sodium 130mmol/L (135-150) Potassium 4.7 mmol/L (3.5-5) Chloride 100mmol/L (98-107) Carbon dioxide 13mmol/L (22-31) Creatinine 420umol/L (65-125) Glucose 1.7mmol/L (4-7.8)
. 2) FBC –Hb 10.9 (11-16.5) TW 21 *10^9 (4-11*) Plt 110 * 10^9 (150-400*) 3)Urine microscopy- WBC >100/HPF(<10) RBC 2 (<2)
Questions • What are the abnormal biochemistry? • What are the causes for her drowsiness? • How would you manage this patient?
1)Whatare the abnormal biochemistry? • Raised urea- 22.4 mmol/L (2.5-7.5) • Raised Creatinine- 420umol/L (65-125) • Hyponatraemia- 130mmol/L (135-150) • Low CO2- 13mmol/L (22-31) • Hypoglycaemia- 1.7mmol ( biochemically low venous/plasma glucose of <2.8mmol/L) • Raised TW- 21 (4-11 *10 ^9) • Raised WBC in urine microscopy- >100/HPF( <10)
2)What are the causes for her drowsiness? • Metabolic disorder - Hypoglycaemia - Hyponatraemia - Dehydration • Infection - septicaemia - Urinary tract infection - Gastroenteritis
Drugs - Glibenclamide • Systemic disorders - Renal disease - Myocardial infarction - Stroke
Diagnosis • Likely to be hypoglycaemia induced by missed meals or anorexia due to underlying sepsis (UTI) and associated with overdosage of glibenclamide.
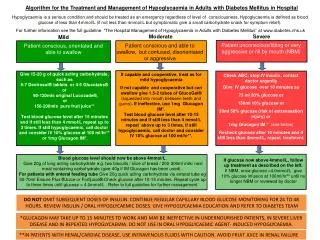
3)How would you manage this patient? 1)(a) IV Dextrose 50% 40-50 ml stat followed by saline flush (b) Infusion of IV D5% or D10% (c) Once alert and can swallow safely, feed with enteral feeds eg. Ensure or Nepro and commence normal diet. (d) Prolonged hypoglycaemia-multiple doses of IV D50% Drowsy-NG tube feeding (e) IM glucagon 1mg not suitable for hypoglycaemia induced by glibenclamide or in liver failure.
2)(a) Recheck capillary BSL 15 mins after initial treatment, then hourly until 2 consecutive BSLs are >10mmol/L. IV Dextrose infusions can then be adjusted downwards stepwise( concentration/rate ), then stopped. (b) Recheck BSL 1 hour after each adjustment. When patient is stable, monitoring can be 2-4 hourly. (c) Keep BSLs between 8-12 mmol/L (d) Glibenclamide associated hypoglycaemia -prolonged monitoring and treatment. - recurrence anticipated.
3) - Septic work-up and treat underlying sepsis. - Give IV dexamethasone 4mg 4 hourly/mannitol/high-dose oxygen to combat cerebral edema and consider CT brain if altered conscious state persists after blood glucose level is returned to normal. - Following recovery, adjust therapy,educate patient,regular monitoring.