Download
1 / 32
370 likes | 646 Vues
Locally Advanced and Metastatic Basal Cell Carcinoma: Medical Oncology Perspective. Karl D. Lewis, MD Associate Professor of Medicine University of Colorado Denver Cutaneous Oncology Program. Basal Cell Carcinoma. Arise from the keratinocytes of the basal layer of the epidermis

E N D
Locally Advanced and Metastatic Basal Cell Carcinoma: Medical Oncology Perspective Karl D. Lewis, MD Associate Professor of Medicine University of Colorado Denver Cutaneous Oncology Program
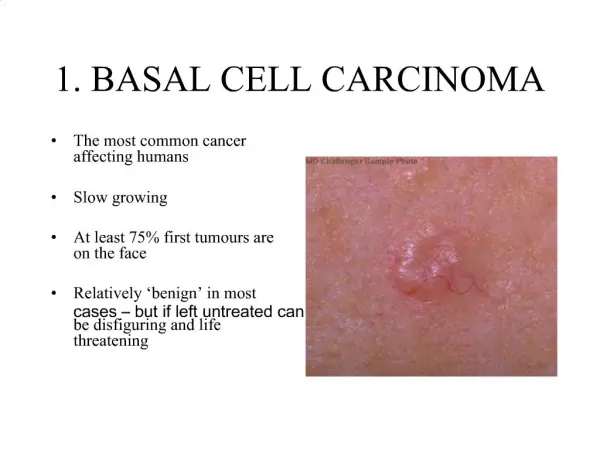
Basal Cell Carcinoma • Arise from the keratinocytes of the basal layer of the epidermis • Generally have a low metastatic potential • However, can be locally aggressive with destruction of skin and surrounding structures • Most common skin cancer in US • Imprecise because no cancer registry • ACS in 2000: ~975,000 cases
BCC - risk factors • UV light exposure • Sun exposure (habits) is most important environmental factor (along with individuals phenotype)
BCC - risk factors • Basal Cell Nevus Syndrome • Robert Gorlin (dentist) identified a syndrome in which multiple abnormalities occur1. • Autosomal dominant • Prevalence varies from 1/57,000 to 1/256,000 • Patients can develop hundreds of BCCs - usually starting by age 35 • Histologic appearance does not differ from sporadic BCCs 1. Gorlin RJ. Nevoid basal-cell carcinoma syndrome. Medicine 1987;66:98-113.
Major Criteria Multiple BCCs or one under 20 yrs Odontogenic keratocysts Palmar/plantar pits Bilamellar calcification of the flax cerebri Bifid, fused or splayed ribs Affected 1st degree relatives Minor Criteria Macrocephaly Congenital malformations (eg, cleft lip) Ovarian fibroma Skeletal abnormalities Medulloblastoma Basal cell nevus syndrome
Bone cysts (mandible) palmer/plantar pitting Bifid ribs
Basal Cell Nevus Syndrome (BCNS) • Positional cloning and subsequent screening identified a spectrum of PTCH mutations in BCNS patients • BCCs develop secondary to activation of target genes of Hh pathway in cells that have lost both normal copies of PTCH
Hedgehog Signaling Pathway The hedgehog pathway is active during embryonic development but dormant after birth Basal cell nevus syndrome: Germline mutation in PTCH gene
Sporadic BCCs • Majority show allelic loss for chromosome 9q22 and inactivating mutations of PTCH • Activating mutations of SMO in 10-20% sporadic BCCs • Suggests abnormal Hh signaling involved in most (all?) BCCs - high levels of Hh target genes such as GLI1
Basal Cell CarcinomaTreatment • Low risk lesions: • Cryosurgery • Electrodessication • Topical therapy: 5-FU or imiquimod • High risk lesions: • Surgical excision • Mohs micrographic surgery • Radiation therapy (cure rates 85-95%)
Basal Cell CarcinomaTreatment • Low risk lesions: • Cryosurgery • Electrodessication • Topical therapy: 5-FU or imiquimod • High risk lesions: • Surgical excision • Mohs micrographic surgery • Radiation therapy (cure rates 85-95%)
Medical Oncologist Role in Treatment of BCC • Historically: little to none • No clinical trials demonstrating chemotherapy benefit • Chemotherapy responses on case-report basis only • NCCN Guidelines: recommend clinical trials (Hhi) for metastatic BCC
Medical Oncologist Role in Treatment of BCC • Metastatic BCC • First case of metastatic BCC reported in 18941 • Since then have been >300 cases reported • Accurate incidence difficult to obtain: no good registry • Estimated rates reported to be: 0.0028% to 0.55%2,3 • However, these data are old and based on single institutions or small subsets • The lower incidence would translate to 1 in 35,000 patients (seems too high considering total number of patients reported in the literature)4,5 • Beadles DF. Trans Pathol Soc 1894. • Paver K et al Australas J Dermatol 1973 • Cade S et al 1940 • Wadhera A et al Dermatol Online J 2006 • Ganti AK et al Cancer Treat Rev 2011
Chemotherapy for BCC • Metastatic • Numerous agents on case-report basis: • Cyclophosphamide, etoposide, 5-FU, MTX, bleomycin, doxorubicin, cisplatin, carboplatin, paclitaxel • Cisplatin (alone or combination) likely most effective: • 12 patients treated with platinum containing regimen1: • 5 CR (3 to 18 months) • 4 PR • 3 SD 1. Carneiro BA et al Cancer Invest, 2006
Chemotherapy for BCC • Problems with case-reports: • No consistent treatment regimen • Dose • Schedule • Timing of response • Selection bias of patients • What prompted treatment vs no treatment • Much more likely to report responders than non-responders • No standardization of response evaluation!!!! • Even though chemo responses seem encouraging it is not known what the true response rate is.
BCC • Since the HH pathway seems to be ubiquitously expressed in BCC, there may be a potential for targeted therapy.
Anomalous development due to disruption of Hedgehog signaling Enabled by the ingenuity of Lynn James, from the US Department of Agriculture, in investigating the curious case of an epidemic of cyclopic lambs in Idaho, 1957 Cyclopamine VeratrumCalifornicum Cyclopic lamb
Genentech: GDC-0449 (Vismodegib) Approved Infinity: IPI-926 (Saridegib) Ph1 Novartis: LDE225 (Erismodegib) Ph2 AstraZeneca: AZD8542 Ph1 BMS: BMS-833923 (XL139) Ph1 Millennium: TAK-441 Ph1 Novartis: LEQ506 Ph1 Hedgehog inhibitors in the clinic
ERIVANCE BCC: Pivotal Phase 2 study in advanced BCC RECIST Metastatic BCC (RECIST-measurable) • Progression • Intolerable toxicity • Withdrawal fromstudy Vismodegib REGISTRATION Compositeendpoint Locally advanced BCC • Locally advanced BCC: • Inoperable • Surgery inappropriate • 1 cm • 2 recurrences after surgery and curative resection unlikely and/or anticipated substantial morbidity and/or deformity from surgery 19 RECIST, Response Evaluation Criteria In Solid Tumors
ERIVANCE BCC: Study Objectives • Primary endpoint: Objective response rate by independent review • Hypotheses tested: • Overall response rate is significantly greater than 10% in patients with mBCC or 20% in patients with laBCC • Secondary endpoints included: • Objective response rate by investigator • Progression-free survival • Duration of response • Absence of residual BCC in patients with laBCC
Vismodegib demonstrates a significant objective response rate in mBCC Sekulic A et al. N Engl J Med. 2012;366:2171-2179. CI, confidence interval; IRF, independent review; INV, investigator review
Maximum decrease in tumor size by IRFMetastatic cohort 100 Partial response Stable disease Progressive disease 50 Change in lesion diameter (%) 0 -50 -100 Sekulic A et al. N Engl J Med. 2012;366:2171-2179. Maximum decrease in size prior to IRF-determined disease progression 22
Vismodegib demonstrates a significant objective response rate in laBCC Sekulic A et al. N Engl J Med. 2012;366:2171-2179.
Maximum decrease in tumor size by IRFLocally advanced cohort 100 Response Stable disease Progressive disease 50 Change in lesion diameter (%) 0 -50 -100 Sekulic A et al. N Engl J Med. 2012;366:2171-2179. Maximum decrease in size prior to IRF-determined disease progression 24
Vismodegib in locally advanced BCC Baseline Week 8 Week 20 Week 16: no BCC on biopsy Sekulic A et al. N Engl J Med. 2012;366:2171-2179. 25
Vismodegib in locally advanced BCC Baseline Week 24 Week 24: residualBCC on biopsy Sekulic A et al. N Engl J Med. 2012;366:2171-2179.
ERIVANCE*(SHH4476g) Phase II Vismodegib in Advanced BCC: Vismodegib in Locally Advanced BCC Baseline Week 32 Week 24: no residual BCC on biopsy Sekulic A, et al. Presented at EADO. 2011 (abstr CO14).
ERIVANCE*(SHH4476g) Phase II Vismodegib in Advanced BCC: Vismodegib in Locally Advanced BCC Baseline Week 8 Week 24 Week 24: no residual BCC on biopsy Sekulic A, et al. Presented at EADO. 2011 (abstr CO14).
Most common adverse eventsAll treated patients (n=104) Sekulic A et al. N Engl J Med. 2012;366:2171-2179. MedDRA, Medical Dictionary for Regulatory Activities
ERIVANCE: 12 Month Update Efficacy Conclusions • At the 12-month update both INV- and IRF-assessed ORRs remained similar to those reported at the primary analysis • Four additional patients became responders • Median DOR remained similar to the primary analysis • For both the mBCC and laBCC cohorts, the median PFS per IRF assessment at the 12-month update was similar to that at the primary analysis • Among patients with laBCC the median PFS by INV was 1.6 months longer than the median PFS at the primary analysis • As of 28 November 2011, median OS was 24.1 months in the mBCC cohort and was not estimable in the laBCC cohort • One-year survival rates at this 12-month update were similar to those at the primary analysis Sekulic A, et al. Ann Oncol. 2012;23(Suppl 9):abstr 1112PD.
Phase 2 BOLT Trial: Investigating Basal Cell Carcinoma Outcomes in LDE225 (Erismodegib) Trial • BCC patients (N=156) • Locally advanced or metastatic disease • Not amendable to radiation therapy, surgery, or other local therapies • Stratification • Stage of disease • Histological subtype (for locally advanced disease) R A N D O M I Z E 2:1 • Treatment continues until: • Disease progression • Intolerable toxicity • Death • Study termination • Withdrawal of consent LDE225 800 mg PO daily LDE225 200 mg PO daily Primary endpoint: ORR Secondary endpoint: TTR, DoR, PFS, OS, safety, PK profile, CRch Estimated completion: September 2014 ORR = overall response rate; TTR = time to tumor response; DoR = duration of response; PFS = progression-free survival; OS = overall survival; PK= pharmacokinetic; CRch = complete histological clearance. Available at: http://clinicaltrials.gov/ct2/show/NCT01327053. Accessed October 11, 2012.
Conclusions • BCC is very common cancer that rarely becomes locally advanced or metastatic (but when it does it is a major problem!). • Cisplatin containing chemotherapy regimens likely has activity: but no clinical trials to guide clinicians. • HHi showing very encouraging activity in clinical trials. • Further supports the concept of molecularly targeted therapies.