Download
1 / 46
470 likes | 696 Vues
Hypothyroidism. Dra Roopa Mehta Departamento de Endocrinología y Metabolismo Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán. Introduction. This is the most common pathological hormone deficiency

E N D
Hypothyroidism Dra Roopa Mehta Departamento de Endocrinología y Metabolismo Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán
Introduction • This is the most common pathological hormone deficiency • The deficiency of thyroid hormones results in a slowing down of metabolic processes • Prevalence 2-3% in the general population • Mean age at diagnosis is mid-50s • Male: Female 1:10
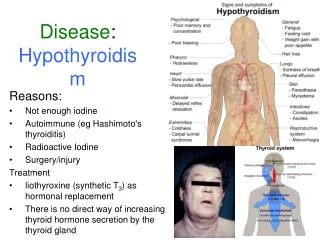
Introduction • Classification: Time of onset: Congenital or acquired Severity: Clinical or subclinical Site of dysfunction: Primary or secondary/tertiary • Pathogenesis: The most characteristic finding is the accumulation of glycosaminoglycans (mostly hyaluronic acid) in interstitial tissue. This results in interstitial edema (e.g. in skin, heart muscle etc.). The accumulation is due to decreased destruction of glycosaminoglycans.
Congenital hypothyroidism • Incidence : 1 in 4000 • Male: Female 1:2 • The most common cause worldwide is endemic iodine deficiency (<100mcg/day) • In areas with sufficient iodine intake: 85% sporadic / 15% hereditary • Thyroid dysgenesis (aplasia, hypoplasia and ectopic gland). (Associated with mutations in the genes for PAX8 and TTF-2 (transcription factors involved in morphogenesis and differentiation of thyroid gland)
Congenital hypothyroidism • Dyshormonogenesis. Defects in thyroid hormone synthesis, secretion or utilization (autosomal recessive). Include mutations in genes for thyroid TSH receptor, thyroid peroxidase gene, iodine transporter and thyroglobulin. Also mutations in genes for transcription factors needed for pituitary thyrotrope differentiation (pit-1, prop-1, HES-X) 3. Failure of thyroid descent- “ectopic” poorly functioning thyroid 4. Maternal radioactive iodine treatment/ antithyroid drugs (propylthiouracil) 5. Transplacental transfer of TSH receptor (blocking) antibody from mother with Hashimotos thyroiditis
Congenital hypothyroidism Symptoms: Jaundice, lethargy, feeding problems, respiratory problems, constipation, hypothermia Signs: • Puffy face, goiter • Protruding tongue (macroglossia) • Hoarse cry • Distended abdomen • Umbilical hernia • Muscle weakness (cannot sit up without help) • Slow reflexes
Congenital hypothyroidism • Diagnosis: Neonatal screening. Heel prick test 24-48 hrs after birth. A low T4 (<6ug/dl) and elevated TSH (>30uU/ml) Marked retardation of bone maturation. Absence of proximal tibial and distal femoral epiphysis suggests hypothyroidism • Treatment: Replacement therapy • Children: growth failure and mental retardation • Adolescents: growth failure and precocious puberty may occur (pituitary hypertrophy)
Primary hypothyroidism • Disease of thyroid characterised by low serum T4 and high serum TSH (above reference values) • In adults >65 years incidence is approx. 10% • Overall incidence in population is 1-2% • Two forms of primary hypothyroidism: • Overt hypothyroidism (low free T4, high TSH) • Subclinical hypothyroidism (normal free T4 and T3, high TSH)
Causes of primary hypothyroidism • Most frequent causes of overt/subclinical hypothyroidism- 1-4 : • Chronic autoimmune (Hashimoto´s) thyroiditis • Thyroid surgery (2-4 weeks following after total thyroidectomy) • Radiation treatment I131 (for treatment of Graves commonly) • Drugs: iodine deficiency or excess, methimazole, propylthiouracil, lithium, amiodarone, interferon alpha • Excessive iodine intake (radiocontrast dye, kelp) • Infiltrative diseases- rare (e.g. hemochromatosis,TB, leukemia, amyloid etc.) • Thyroiditis
Chronic autoimmune thyroiditis (Hashimoto´s) • Most common cause in iodine sufficient areas • Male: Female 1:7 • Goitrous and atrophic forms- differ in extent of lymphocytic infiltration, fibrosis, and thyroid follicular cell hyperplasia • Hypothyroid or euthyroid • Associated autoimmune diseases: polyglandular syndromes 1 and 2, vitiligo, pernicious anemia etc.
Chronic autoimmune thyroiditis (Hashimoto´s) • Pathogenesis: • Cell and antibody mediated destruction of thyroid gland • Diffuse lymphocytic infiltrate + circulating autoantibodies Lymphocytes become sensitized to thyroid antigens resulting in formation of autoantibodies: thyroperoxidase (TPO in 95%), thyroglobulin (Tg in 60%) and TSH receptor blocking antibody (TSH-R ) • Genetic predisposition: HLA-DR5, HLA-B8 histocompatibility antigens
Yellow arrows = lymphoid aggregates with germinal centers • Red arrows = diffuse lymphocytic infiltrate • Blue arrows = small atrophic follicles lined by hurtle cells
Drugs causing hypothyroidism • Methimazole/ Thiamazole: Block biosynthesis of thyroid hormones by inhibiting production of thyroid peroxidase • Propylthiouracl: In addition blocks peripheral conversion of T4-T3 • Iodine: Deficiency and excess (inhibition of iodide organification and T4 and T3 synthesis esp. with underlying autoimmune disease) • Lithium: interferes with release of thyroid hormones, causing transient elevation of TSH in a third and persistent hypothyroidism in 10% (esp. with underlying autoimmune disease) • Amiodarone (iodine containing): inhibits thyroid hormone production and peripheral conversion (esp. with underlying autoimmune disease) 22% with overt or mild hypothyroidism in one study. Long half life (40-100d)
Transient primary hypothyroidism • Subacute thyroiditis (granulomatous/Quervains) viral in origin (coxackie, mumps, adenovirus) fever/malaise and tender thyroid unilateral hard mass • Lymphocytic thyroiditis (painless/silent/postpartum) Usually in postpartum women (2-12 weeks) (8% of postpartum women) painless thyroid enlargement 80% with elevated TPO antibodies
Transient primary hypothyroidism • Both conditions have low RAIU • Both present with transient hyperthyroidism (4-8 weeks) followed by a euthyroid phase. Patients may remain euthyroid or progress to a hypothyroid phase that lasts 2-3 months followed by recovery (85% SAT, 75% LT) • Patients often need temporary replacement therapy • In LT, persistent thyroid abnormalities such as goiter and/or frank hypothyroidism occur in one third of patients. Recurrence probable in subsequent pregnancy
Subclinical hypothyroidism • Asymptomatic state (subclinical symptoms) with normal serum and free T4 but elevated TSH • Prevalence 4-8.5%; up to 15% in women >60 years • Causes same as for overt hypothyroidism- commonly chronic autoimmune thyroiditis, post radiation, inadequate replacement therapy • Continuum between euthyroidism and hypothyroidism • The distinction between a normal TSH and elevated TSH is arbitrary • Is treatment recommended???
Subclinical hypothyroidism CONSEQUENCES AND RISKS • Symptoms of hypothyroidism; weight gain • Neuropsychiatric symptoms: depression, loss of memory • Neuromuscular symptoms: >CPK, weakness, peripheral neuropathy • Coronary artery disease (atherosclerosis) and cardiac dysfunction (reduced myocardial contractility); >CRP • Elevated total and LDL cholesterol • Progression to overt hypothyroidism
Subclinical hypothyroidism • Arguments for treatment Reduction of risk for CV disease (improve myocardial function and lower LDL), prevention of goiter growth and improvement in subclinical symptoms • Arguments against treatment Cost, lifelong commitment to medication in asymptomatic patients, risk of angina and arrhythmias in susceptible patients
Subclinical hypothyroidism • In patients with TSH levels >10mU/L- Treat with T4 to reduce CAD risk and prevent progression to overt hypothyroidism (especially in patients with high serum TPO antibody titers and >65years) • TSH between 4.5-10mU/L: some studies have shown risk for CAD and presence of hypothyroid symptoms
Subclinical hypothyroidism • When evaluating such patients take into account: Clinical manifestations (symptoms and/or goiter) Presence of TPO antibodies Age Women of reproductive age with infertility or pregnant Progression of TSH levels with time (can normalise) • TSH between 3-4.5mU/L: only significant risk appears to be progression to overt hypothyroidism over time
Secondary and Tertiary hypothyroidism • Account for <1% of patients with hypothyroidism (adulthood or childhood) • Inappropriately low or normal TSH concentration (in presence of low T4 and T3) • Secondary hypothyroidism caused by TSH deficiency (often pituitary tumors, Sheehan's syndrome, surgery/radiotherapy) • Tertiary hypothyroidism caused by TRH deficiency (hypothalamic damage from tumors, trauma, radiation, infiltrative diseases) • Secondary and tertiary hypothyroidism cannot be distinguished by biochemical tests- MRI should be requested (mass lesion), other hormone deficiencies
Clinical manifestations of hypothyroidism • Depends on degree of hormone deficiency (overt, subclinical) • Depends on speed of development of hormone deficiency (gradual, better tolerated)
SYMPTOMS Fatigue/ lethargy Non-pitting edema of face (periorbital edema) and hands Paraesthesias Deep hoarse voice Loss of memory/<Concentration Somnolence/ Cold intolerance Depression Constipation (ileus) Arthralgia/ Myalgia with proximal weakness Dry skin and hair loss Weight gain /Carpal tunnel synd. Menstrual irregularities Growth retardation in children Deficiency of other hormones SIGNS Yellowish tinge to skin (>carotenes) Bradycardia Systemic arterial hypertension Goiter or small thyroid Dry, cold skin Slow reflexes Signs and symptoms
Clinical Manifestations • CARDIOVASCULAR SYSTEM: Impaired muscle contraction, bradycardia and reduced cardiac output. Hypertension- >Peripheral vascular resistance Cardiac enlargement due to interstitial edema but often due to pericardial effusion Low voltage complexes on ECG • RESPIRATORY SYSTEM: Hypoventilation -Respiratory muscle weakness -Impaired ventilatory response to hypoxia and hypercapnia -Sleep apnea (retention of CO2)
Clinical Manifestations • GASTROINTESTINAL SYSTEM: Slowing of peristalsis leads to constipation • ANEMIA: Usually normochromic, normocytic anemia- • Impaired Hb synthesis due to thyroxine deficiency • Iron def. due to menorrhagia and impaired intestinal absorption • Folate deficiency from impaired intestinal folate absorption • Pernicious anemia with Vit-B12 def. megaloblastic anemia
Clinical Manifestations • REPRODUCTIVE SYSTEM: Oligo / amenorrhea (16%) Menorrhagia (7%) Hyperprolactinemia occurs because of absence of inhibitory effect of thyroid hormone on prolactin secretion and causes galactorrhea and amenorrhea • NEUROMUSCULAR SYSTEM: Carpal tunnel syndrome >CPK- muscle cramps, proximal weakness Slow relaxing reflexes
Clinical Manifestations • RENAL SYSTEM: Decreased glomerular filtration rate -Impaired ability to excrete a water load (hyponatremia) • SKIN AND HAIR: Glycosaminoglycan, mainly hyaluronic acid, accumulate in skin and tissues causing retention of sodium and water- puffy skin Reduced blood flow and calorigenesis- hypothermia and decreased sweating Carotenemia. Loss of lateral eyebrows
Clinical Manifestations • METABOLIC ABNORMALITIES: Hyponatremia (<free water clearance because of inappropriate ADH production) Hyperlipidemia: reduced number of lipoprotein lipase receptors, reduced degradation of lipoproteins and reduced lipoprotein lipase activity (4.2% of patients with hyperlipidemia • Hypercholesterolemia 56% • Hypertriglyceridemia 1.5% • Mixed hyperlipidemia 34%) Hyperhomocystinemia
Diagnostic tests • Clinical evaluation • Measure T4 (total or free), T3 (total or free) and TSH • Thyroid antibodies: anti TPO anti Tg • Cerebral MRI / CT when searching for mass lesion (Enlargement of pituitary also occurs in primary hypothyroidism due to hyperplasia of thyrotropes) • TRH test for diagnosis of central hypothyroidism
Hypothyroidism Suspicion of hypothyroidism Thyroid function tests Hypothyroidism Normalsize or small thyroid Goiter Increased TSH TSH normal or reduced Central hypothyroidism Primary hypothyroidism T3 + T4 + TSH T3 + T4 +TSH nl /
Hypothyroidism Hypothyroidism Primary hypothyroidism Central hypothyroidism Anti thyroid AB+ Anti thyroid AB- Drugs: Lithium Amiodarone Etc. Surgery or tx 131I Postpartum thyroiditis Autoimmune thyroiditis Pituitary MRI or CT TRH test
Treatment • Normal metabolic state should be restored gradually as rapid increase in metabolic rate may precipitate cardiac arrhythmias • Thyroxine (100mcg) or mixture of T3(20mcg) and T4(100mcg) • Exclude adrenal insufficiency before initiating tx. • Given 1x daily in morning (T4 t1/2=7days)- fasting • In elderly, with ischemic heart disease, initial dose 25ug; increased gradually at 4 week intervals • Monitor improvement in clinical symptoms and normalization of TSH • Secondary hypothyroidism- free T4 used for monitoring response to tx.
Factors that increase the requirement for T4 • Pregnancy, Estrogen therapy, Weight gain • Drugs which increase catabolism of T4: Rifampin, Carbamazepine, Phenytoin, Phenobarbitol • Malabsorption or increased excretion of T4: Gastrointestinal disorders, Impaired acid secretion • Drugs which interfere with T4 absorption: Ferrous sulfate, Cholestyramine or colestipol, Sucralfate Aluminum hydroxide gels, Calcium Carbonate, Sertraline Raloxifene, Omeprazole • Nephrotic syndrome • Progressive thyroid dysfunction
Potential causes of TSH elevation in thyroxine-treated patients with primary hypothyroidism • Suboptimal dosing: Inadequate prescribed dosage, noncompliance, dispensing error (incorrect dose or formulation change) • Progressive decrease in endogenous thyroxine production: Autoimmune thyroiditis, Previous thyroid irradiation • Reduced thyroxine absorption Drug interactions: Iron, Calcium carbonate, Cholestyramine, Aluminum hydroxide gel, Sucralfate, dietary soy and fiber Comorbid conditions: Disorders causing malabsorption - eg, celiac disease, previous small bowel surgery • Increased thyroxine clearance Drug interactions: Phenytoin, Carbamazepine, Phenobarbitol etc. Coexisting conditions: Pregnancy, Nephrotic syndrome • Other: Postmenopausalhormone replacement therapy
Myxedema Coma • End-stage of untreated hypothyroidism- medical emergency • Clinical manifestations: Decreased mental status, hypothermia, bradycardia, hypotension, hypoventilation (>pCO2), hypoglycemia, typical myxedematous facies and skin, hyponatremia (impaired water excretion and disordered regulation of vasopressin secretion), slow relaxing reflexes, coma and death Precipitated by intercurrent illness such as infection, stroke or CNS depressants If untreated 100% mortality
Myxedema Coma • Identify and treat intercurrent illness • Antibiotic therapy after blood cultures • Passive external rewarming for hypothermia. 0.5degrees celsius / hr • Warm humidified O2, mechanical ventilation if necessary and cardiac monitor for arrhythmias • Correct hyponatremia (fluid restriction), hypotension and hypoglycemia • Take blood for TFTs and cortisol before starting tx. If hypocortisolemic start hydrocortisone • T4 300-500ug iv followed by 50-100ug / daily If no response within 24-48hrs, T3 10ug iv 8 hourly
CASO CLINICO • Mujer de 27 años con antecedentes familiares de enfermedad tiroidea (una tía materna con enfermedad de Graves y una hermana con hipotiroidismo) • Ciclos menstruales regulares hasta hace dos años, actualmente 40-60 x 2-3 • Un año con piel seca, fatiga y estreñimiento • EF: peso 68 kg (previo 63), TA 130/70 FC 58 x min • Edema bipalpebral, piel seca, tiroides palpable pequeña, ROTS lentos
CASO CLINICO PFT’s CT3 0.65 (0.75 -1.25) T31 nmol/l (1.16 -3.86) T465 nmol/l (77.2-154.4) TSH 10 mU/l (0.5-3.5) Tg 5 ng/ml(0-30) AcTPO 1:25,000 (negativos) AcTg negativos (negativos)
CASO CLINICO • A 29 year old woman with a history of a diffuse goiter with normal TFTs. She gave birth to a healthy baby 4 months ago. A month ago she developed symptoms of tremor, irritability and mild heat intolerance. T4 14.3ug/dl (4.5-12) TSH 0.03mIU/ml (0.32-5) Today she has fatigue, dry skin, somnolence and difficulty concentrating at work On examination, 92kg, 130/70, no lid lag or exophthalmus. Thyroid diffusely enlarged. No bruit. Family history of Graves disease
CASO CLINICO • Does this woman have Graves disease? New TFTs: free T4 0.6ng/dl (0.7-2.2) T3 78ng/dl (80-200) TSH 27.3mIU/ml (0.32-5) • What is the diagnosis? How is it treated?
CASO CLINICO • A 51 year old man presents with a 5 week history of right sided neck pain radiating to right ear. He has had a mild URTI 7 weeks ago. He is physically fit with a normal pulse of 50; but in last 2 weeks this has risen to 70. He feels nervous and irritable. On examination, slightly enlarged tender thyroid gland, with no lymphadenopathy. TFTs: free T4 1.9ng/ml (0.7-2.2) TSH 0.03mIU/ml (0.32-5.00) U/S diffusely enlarged thyroid gland RAU scan 2hr uptake 1.9% 24hr 2.3% (Norm=20%)
CASO CLINICO • What disorder does this man have? • Appropriate treatments include: • Surgery • Prophylthiouracil or methimazole • Propranalol • Ibuprofen • Predisolone • Radioactive iodine
CASO CLINICO • 72 year old woman brought to ER in respiratory arrrest (respiratory frq-6). Not responsive. Family says she has been disorientated last 2 weeks. PMH: depression, hypothyroidism, and peptic ulcer disease. (captopril, levothyroxine, ranitidine) • On examination minimally responsive. Thin woman. Cool dry skin. Bilateral crepitations on pulmonary examination Temperature 95 farenheit • Intubated and mechanically ventilated Na 119mmmol/l (135-145) K 3.7mmol/l (3.5-5.2)
CASO CLINICO Arterial pH 7.31 (7.35-7.45) Plasma osmolality 258mOsm/kg (270-290) Toxicology negative What tests would you ask for? Why might hyponatremia be present? How should this patient be treated?