Download
1 / 36
370 likes | 776 Vues
EMS Management of Hypothermia November 2013 CE. Erika Ball, RN, BSN. Objectives: Understand the physiology of hypothermia EMS considerations for the hypothermic patient Mechanisms of heat loss. Clinical indications of hypothermia Degrees of hypothermia Treatment and rewarming

E N D
EMS Management of HypothermiaNovember 2013 CE Erika Ball, RN, BSN
Objectives: • Understand the physiology of hypothermia • EMS considerations for the hypothermic patient • Mechanisms of heat loss • Clinical indications of hypothermia • Degrees of hypothermia • Treatment and rewarming • Other considerations in hypothermia Bledsoe, 2013.
Temperature regulation: • Happens in the hypothalamus • The hypothalamus is the body’s “thermostat” • The body has thermo sensors in the skin the mucosa, and in certain deeper structures in the body • The hypothalamus works as a regulator for shivering and sweating, depending on the environmental stimulus (excessive cold or heat). Bledsoe, 2013.
There are two rates the temperature regulation system effects: • Basal Rate- the normal resting rate for the CORE of the body (deep internal temperature) • Metabolic Rate- reactive adjustment to the environment to maintain a continual core temperature Bledsoe, 2013.
Normal body temperature is 98.6o F or 37o C • Hypothermia definition: • Decrease (unintentionally) in CORE temperature greater than 3.5 degrees from the basal temperature Bledsoe, 2013.
Conduction • Convection • Radiation • Evaporation • Respiration Mechanisms of heat loss Bledsoe, 2013.
Conduction: • Direct contact with a cooler object • Heat loss happens in the direction of the high temperature to the low temperature Bledsoe, 2013.
Convection: • Air temperature causes heat loss • Radiation: • Infrared rays cause heat loss • Infrared heat loss is always happening until temperatures reach molecular standstill (called absolute zero) Bledsoe, 2013.
Evaporation: • Water evaporation causes heat loss • This phenomenon can happen from the skin or water evaporating in the air as we breathe Bledsoe, 2013.
Respiration: • A combination of convection, radiation, and evaporation occurs during the respiratory process, causing further heat loss Bledsoe, 2013.
Body composition • Thermoregulatory response (shivering ability/ heat production) • Clothing/insulation • Water or air temp and conditions • Medications or intoxication • Age • Health • Extended exposure • Associated Injury What effects the cooling process? Bledsoe, 2013.
Mechanisms for heat conservation: • Vasoconstriction of peripheral blood vessels • Skin becomes pale and cool • Goose bumps (unknown why this truly happens, some speculate this is an evolutionary remnant*) Bledsoe, 2013.
Hypothermia results from: • Insufficient heating mechanisms • Severe cold stress (exertion with cold exposure) Bledsoe, 2013.
Degrees of hypothermia: • MILD: 95- 89.6 F • Thermoregulatory mechanisms are still operating fully • MODERATE: 89.6- 82.4 F • Effectiveness of thermoregulatory mechanisms diminish until they fail • SEVERE: Lower than 82.4 F • Loss of consciousness • No more shivering • pH balance disrupted • Susceptible to V Fib or asystole Bledsoe, 2013.
Cold response progression Bledsoe, 2013.
1.Short-term (Cold shock response) 2. Midterm (Loss of performance) 3. Long-term (development of hypothermia) Progression of hypothermia Bledsoe, 2013.
Short-term: Cold Shock response Bledsoe, 2013.
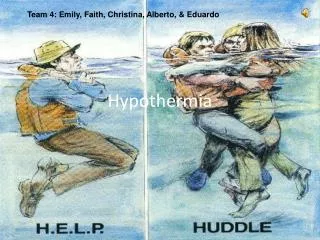
Generally in water • First 3-4 minutes of immersion (with head out of the water) • Peripheral vasoconstriction • Panic • Gasp reflex • Hyperventilation • Tachypnea • Vagal cardiac arrest and subsequent drowning (Polar bear plunge!!) Cold-shock response Bledsoe, 2013.
IF they survive the cold-shock, this is the next 30 minutes of progression • Neuromuscular activity and loss of motor control • If the neuromuscular mechanisms fail, individual can not execute survival procedures (grabbing life preserver) and individual will drown Mid-term Bledsoe, 2013.
Development of hypothermia process • Mild • Moderate • Severe Long-term Bledsoe, 2013.
Shivering • Lethargy • Lack of coordination • Pale cool skin • Early stages witness rise in BP, heart rate, and respiration Mild hypothermia Bledsoe, 2013.
Shivering ceases • Arrhythmias can occur • Cardiac arrest • Voluntary muscle control loss • Hypotension • Pulse and respirations become undetectable Severehypothermia Bledsoe, 2013.
Initial treatment: • Remove any wet clothing • Stop cooling process with blankets and elements • Keep patient in supine to prevent further hypotension • Handle patient gently (skin is fragile) • Establish cardiac rhythm EMS Hypothermia Treatment Bledsoe, 2013.
PR interval can become longer (1st degree heart block) • This progresses to a prolonged QRS and QT • “J” waves, or Osborne waves, can occur under a core temperature of 90OF EKG in Hypothermia- Cardiac review Bledsoe, 2013.
J waves are most frequent in leads II and V6 • These waves become larger in size as the patient’s core temperature decreases EKGinHypothermia Bledsoe, 2013.
Rewarming the patient Bledsoe, 2013.
Active rewarming: • Mild hypothermia- external methods • Blankets • Heat packs (in axilla and groin) • Mild Hypothermia- internal rewarming • Warm IV fluids • If the patient is still shivering, rewarming should occur quickly Mild hypothermia rewarming Bledsoe, 2013.
External: • Warm blankets • Heat packs (again, groin and axilla) • Internal • Warmed IV Fluid • Warm, humidified oxygen • Best done in the ER, where protocol exists for slowly rewarming the patient Severe Hypothermia Rewarming Bledsoe, 2013.
EMS should use caution in rewarming the patient due to peripheral reflex dilation • Patient’s rewarming sometimes causes a hypotension and can precipitate V Fib • This is why warm packs in the groin and axilla warm the core rather than the extremities Rewarming shock Bledsoe, 2013.
Region VII SMO for Hypothermia Bledsoe, 2013.
DO NOT give any drugs to these patients! • Assess the pulse for a full 30-45 seconds • May attempt defibrillation x1 Cardiac Arrest Bledsoe, 2013.
Morphine: Medication of the month related to Hypothermia Bledsoe, 2013.
Morphine • Binds with opioid receptors to produce narcotic analgesia • CNS depressant • Causes peripheral vasodilation • May be given in 5 mg increments for severe pain (blood pressure permitting) for a dose of 5-10 mg in hypothermia, at the discretion of the ECRN/ MD. • Contraindications: • Respiratory depression, shock, hypotension, known sensitivity or allergy. Use with caution in bronchial asthma, respiratory insufficiency, head trauma Medication of the month related to Hypothermia Bledsoe, 2013.
Thank you for your time and attention! • The 2014 CE calendar will be available early in December! • We welcome your suggestions! Bledsoe, 2013.
References Bledsoe, B. 2013Prehospital management in the 21st century. Giesbrecht, G., 2013. Prehospital treatment of hypothermia. Expedition Medicine. Region VII Emergency Medical Service Systems Standing Medical Orders, 2011 Bledsoe, 2013.