Download
1 / 12
120 likes | 298 Vues
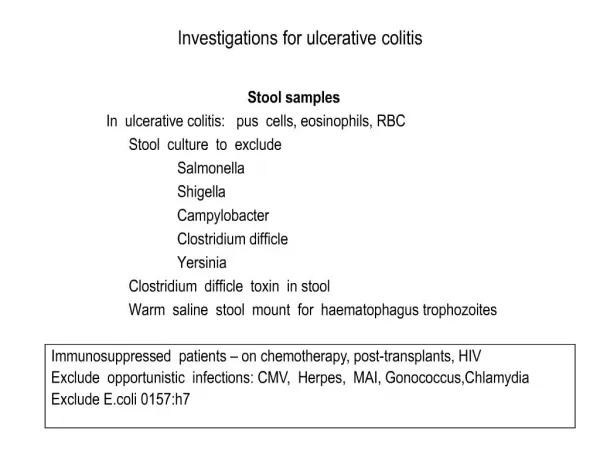
Clinical Guidelines for the Medical Management of Left-Sided Ulcerative Colitis and Ulcerative Proctitis. Miguel Regueiro, MD, Edward V. Loftus, Jr, MD, A. Hillary Steinhart, MD, and Russell D. Cohen, MD, FACG, AGAF Inflamm Bowel Dis, Volume 12, Number 10, October 2006.

E N D
Clinical Guidelines for the Medical Management of Left-Sided Ulcerative Colitis and Ulcerative Proctitis Miguel Regueiro, MD, Edward V. Loftus, Jr, MD, A. Hillary Steinhart, MD, and Russell D. Cohen, MD, FACG, AGAF Inflamm Bowel Dis, Volume 12, Number 10, October 2006
Ulcerative Colitis and Proctitis:Background • UC incidence 2.2-14.3/100,000 person years in North America1 • UC usually presents with disease limited to the distal or left colon1,2 • left-sided UC (L-UC): disease distal to the splenic flexure • ulcerative proctitis (UP): limited to the rectum • ulcerative proctosigmoiditis (UPS): limited to rectosigmoid 1) Loftus EV. Gastroenterology 2004;126:1504-1517; 2) Langholz E. Dan Med Bull 1999; 46: 400-415.
Why L-UC Matters? • L-UC generally amenable to rectally administered (topical) therapy • Topical therapy works more effectively1-3 and more rapidly3 than oral • Emerging data suggest that early, aggressive treatment of UC may prevent or delay proximal extension4 1) Gionchetti P, Rizzello F, Venturi A, et al. Dis Colon Rectum 1998; 41: 93-97. 2) Safdi M, DeMicco M, Sninsky C, et al. Am J Gastroenterol 1997; 92: 1867-1871. 3) Kam L, Cohen H, Dooley C, Rubin P, Orchard J. Am J Gastroenterol 1996; 91: 1338-42 4) Pica R, Paoluzi OA, Iacopini F, et al. Inflamm Bowel Dis 2004; 10: 731-736.
Treatment of Active UP • Topical therapy preferred treatment • Corticosteroids and5-ASAs available in many forms • suppositories reach the upper rectum • enemas reach splenic flexure and the distal transverse colon Proximal distribution of topical preparations Adapted with permission from: Marshall JK, Irvine EJ. Am J Gastroenterol 2000; 95: 1628-1636.
Treatment of Active UP • 5-ASA suppositories first-line therapy1 • highly effective • well-tolerated • Topical 5-ASAs superior to topical corticosteroids in randomized trials2-6 • For patients intolerant of or unresponsive to topical 5-ASA, topical corticosteroids are an alternative1 1) Regueiro M, Loftus EV Jr, Steinhart AH, Cohen RD; Inflammatory Bowel Disease Center. Inflamm Bowel Dis. 2006. 10:972-8. 2) Mulder CJ et al. Eur J Gastroenterol Hepatol 1996; 8: 549-53. 3) Lemann M et al. Aliment Pharmacol Ther 1995; 9: 557-562. 4) Gionchetti P et al. J Clin Gastroenterol 2005; 39: 291-297. 5) Lucidarme D et al. Aliment Pharmacol Ther 1997; 11: 335-340. 6) Farup PG et al. Scand J Gastroenterol 1995; 30: 164-70.
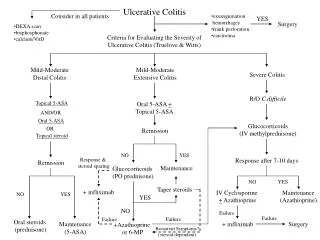
UP Management Algorithm Confirmed ulcerative proctitis (symptoms + endoscopic evidence of mucosal Inflammation not extending above the rectum) Rectal (topical )5-ASA – 1 g/d as suppository (1st Line) 5-ASA 1 – 4 g/d is also effective as liquid enema or foam CLINICAL RESPONSE NO RESPONSE Consider Maintenance Therapy: Rectal 5-ASA suppositories (500 – 1000 mg) 3 times weekly or every second day Add Oral 5-ASA (2.4 – 4.8 g/d) and/or rectal corticosteroid therapy as suppository, enema or foam Frequent / repeated flares Increase maintenance suppository therapy to daily OR Oral 5-ASA 2-4 g/d Colonoscopy to examine for proximal disease progression beyond rectum Treat for Refractory Disease as described elsewhere
Treatment of Active L-UC • Topical 5-ASAs effective for active L-UC • Topical corticosteroids effective alternative for patients intolerant of or unresponsive to 5-ASAs • Combination therapy for patients without adequate response to topical monotherapy • topical 5-ASA and topical corticosteroid, or • oral and topical 5-ASAs • Oral corticosteroids reserved for patients not responding to topical therapies and/or oral5-ASAs 1) Mulder CJ et al. Eur J Gastroenterol Hepatol 1996; 8: 549-53. 2) Safdi M et al. Am J Gastroenterol 1997; 92: 1867-1871. 3) Rizzello F et al. Aliment Pharmacol Ther 2002; 16: 1109-1116. 4) Marteau P et al. Gut 2005; 54: 960-965.
L-UC Management Algorithm Confirmed left-sided ulcerative colitis (symptoms + endoscopic evidence of mucosal inflammation extending beyond the rectum but not extending above the splenic flexure (approximately 60cm)) Consider adding Rectal (topical) 5-ASA: 1-4 g/d as a liquid enema (foam or gel may be used if PS*) Oral 5-ASA 2.4 to 4.8 g/d, or equivalent Clinical Response Insufficient Response Worsening Stop 5-ASA. Start hydrocortisone liquid enema 100 mg qhs. (if PS*, can use hydrocortisone acetate foam 10% qd-bid) See Maintenance Algorithm Insufficient Response Add oral prednisone 40 mg/d or equivalent Clinical Response Insufficient Response See Refractory UC Algorithm *PS = proctosigmoiditis; inflammation limited to rectum and sigmoid.
Maintenance of Remission • UP • Topical 5-ASAs preferred maintenance medication • L-UC • Topical 5-ASA maintains remission in most patients1-3 • Patients achieving remission with combination oral/topical 5-ASA therapy should continue combined therapy for maintenance4 • Oral 5-ASA effective alternative to topical for maintenance • No role for oral corticosteroids in maintenance 1) Hanauer SB et al. Am J Gastroenterol 2000; 95: 1749-1754. 2) Marteau P et al.Gut 1998; 42: 195-199. 3) D’Albasio G et al. Dis Colon Rectum 1990; 44: 394-7. 4) S’Albasio G. et al. Am J Gastroenterol 1997; 92: 1143-1147.
L-UC Maintenance Algorithm Response or Remission Successfully Induced by Following Agent: Change to Intravenous Corticosteroids Oral Corticosteroids Topical Corticosteroids Change to Add mesalamine or corticosteroid enemas (*if PS, can use foam or gel) AND maximum dose of oral 5-ASA. Taper prednisone Consider adding Relapse Oral 5-ASA 1.6 to 4.8 g/d, or equivalent 5-ASA enema (foam or gel if PS*) See Refractory UC Algorithm Continue 5-ASA agents indefinitely Relapse Long-term maintenance Patient may prefer to taper off either oral or rectal agent. Oral 5-ASA + enemas dosed twice weekly effective in some patients. See Induction Algorithm *PS = proctosigmoiditis; inflammation limited to rectum and sigmoid.
Refractory UP and L-UC • Induction of remission • Infliximab1-4 • Cyclosporine effective for acute management5-7 • toxicity limits its long-term use • For patients failing proven regimens • Nicotine and/or antibiotics may be tried • Surgery may ultimately be necessary • Maintenance of remission • Azathioprine/ 6-mercaptopurine, infliximab may be required in corticosteroid dependent disease 1) Sands BE et al. Inflammatory Bowel Diseases 2001;7(2):83-88. 2) Probert CS et al. Gut 2003;52:998-1002. 3) Jarnerot G et al. Gastroenterology 2005;128;1805-1811. 4) Regueiro M et al. J Clin Gastroenterol. 2006 Jul;40(6):476-81. 5) Sandborn W. Inflamm Bowel Dis 1995;1:48-63. 6) Cohen R et al. Am J Gastroenterol 1999;94:1587-92. 7) Lichtiger S et al. N Engl J Med 1994;330:1841-5.
Refractory UP/L-UC Algorithm Review medication compliance Exclude concomitant NSAID use See Maintenance Algorithm Response No response Trial of 5-aminosalicylate cessation and re-challenge (exclude hypersensitivity) No response Colonoscopy with biopsies Stool C. difficile toxin and bacterial culture (Exclude proximal extension, Crohn’s disease, and viral/bacterial superinfection) Response No response ? ? Azathioprine 2-2.5 mg/kg daily or 6-mercaptopurine 1-1.5 mg/kg daily Ciprofloxacin/ metronidazole (efficacy not established) Transdermal nicotine (ex-smokers) No response No response No response Infliximab 5 mg/kg IV induction (0, 2, 6 weeks) Response No response Response Discontinue after 1-2 mos. If relapse continue as maintenance. Infliximab 5 mg/kg IV every 8 weeks Surgery