Download
1 / 43
990 likes | 4.13k Vues
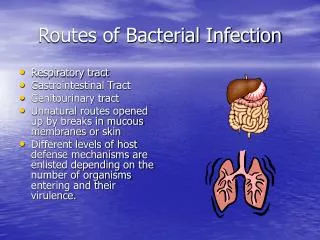
Bacterial Skin Infection. By Prof. Ashraf Al-Sawy MD. Staph. Aureus Infection. Direct infection of skin : impetigo, ecthyma , folliculitis , furunculosis , carbuncle, sycosis . Secondary infection: eczema, infestations, ulcers, …etc.

E N D
Bacterial Skin Infection By Prof. Ashraf Al-Sawy MD
Staph. Aureus Infection • Direct infection of skin :impetigo, ecthyma, folliculitis, furunculosis, carbuncle, sycosis. • Secondary infection:eczema, infestations, ulcers, …etc. • Effect of bacterial toxin:staph.-associated scalded skin syndrome (SSSS), toxic shock syndrome.
strepto. Infection (GAS)(gp A streptococci) • Direct inf. of skin or subcut. tissue:Impetigo, ecthyma, cellulitis, vulvovaginitis, perianal inf., strepto. ulcers, blistering distal dactylitis, necrotizing fasciitis. • 2ry inf.:eczema, infestations, ulcers, …etc.
Tissue damage from circulating toxin:scarlet fever, toxic shock-like syndrome. • Skin lesions attributed to allergic hyper-sensitivity to strepto. antigens:erythemanodosum, vasculitis. • Skin dis. provoked or influenced by strepto. inf.:psoriasis especially guttate forms.
Acute contagious skin infection caused mostly by staph. Aureus and strept. • Affects children mainly esp. in summer times.
Clinical types • 1- Non-bullous impetigo: • Caused by staph., strept. or both organisms. • 2- Bullous impetigo: • Caused by staph aureus.
Non-bullous Impetigo • Staph. aureus or gp A stretp. (GAS) or both “mixed infections”. • May arise as 1ry inf. or as 2ry inf. of pre-existing dermatoses, e.g. pediculosis, scabies & eczemas. • An intact st. corneum is probably the most important defense against invasion of pathogenic bacteria.
A thin-walled vesicle on erythematous base, that soon ruptures & the exuding serum dries to form yellowish-brown (honey-color) crusts that dry & separate leaving erythema which fades without scarring. • Regional adenitis with fever may occur in severe cases.
Sites:Exposed parts eg. face & extremities. Scalp (in pediculosis). Any part could be affected except palms & soles. • Complications:Post-streptococcal acute glomerulo-nephritis “AGN” especially in cases due to strepto. pyogenes M. type 49.
Varities: • Circinate impetigo:with peripheral extension of lesion & healing in the center.
Crusted impetigo: • on the scalp complicating pediculosis. Occipital & cervical LNs are usually enlarged & tender.
Ecthyma (ulcerative impetigo):adherent crusts, beneath which purulent irregular ulcers occur. Healing occurs after few wks, with scarring.
Bullous Impetigo • Age: all ages, but commoner in childhood & newborn (impetigo neonatorum). • Site:face is often affected, but the lesions may occur anywhere, including palms & soles.
The bullae are less rapidly ruptured (persist for 2-3 days) & become much larger. The contents are at first clear, later cloudy. After rupture, thin, brownish crusts are formed.
Treatment of impetigo: • Treatment of predisposing causes:e.g. pediculosis & scabies. • Remove the crusts:by olive oil or hydrogen peroxide. • Topical antibiotic:e.g. tetracycline, bacitracin, gentamycin, mupiracin (Bactroban®), Fusidic acid (Fucidin®).
Systemic antibiotics are indicated especially in the presence of fever or lymphadenopathy, in extensive infections involving scalp, ears, eyelids or if a nephritogenic strain is suspected, e.g. penicillin, erythromycin & cloxacillin. • Azithromycin (Zithromax®) 2 caps 500 mg daily for 3 days in adults. • In erythromycin-resistant S. aureus: amoxicillin + clavulanic a. (Augmentin®) 25 mg/kg/day.
inflammatory disease of the hair follicles, which may be infectious or non-infectious.
Superficial Folliculitis (Bockhart’s Impetigo)
a dome-shaped pustule at the orifice of a hair follicle that heals within 7-10 days.
Caused by staph aureus and affects mainly extremities and scalp. • Topical steroids are a common predisposing factor.
Recurrent red follicular papules or pustules centered on a hair, usually remain discrete over the beard or upper lip, but may coalesce to produce raised plaques studded with pustules. • DD: pseudofolliculitis of the beard, T. barae.
from penetration into the skin of sharp tips of shaved hairs.
It is a staphylococcal infection similar to, but deeper than folliculitis & invades the deep parts of the hair folliculitis. • Occasionally several closely grouped boils will combine to form a carbuncle. The carbuncle usually occurs in diabetic cases. The site of election is the back of the neck.
Cellulitis is an infection of subcutaneous tissues. • Ersipelas:It’s due to infection of the dermis & upper subcutaneous tissue by gp A streptococci. The organism reaches the dermis through a wound or small abrasion. It is regarded as a superficial “dermal” form of cut. cellulitis.
Erythema, heat, swelling and pain or tenderness. • Fever and malaise which is more severe in erysipelas. • In erysipelas: blistering and hemorrhage. • Lymphangitis and lymphadenopathy are frequent.
Edge of the lesion: well demarcated and raised in erysipelas and diffuse in cellulitis.
Complications • Recurrences may lead to lymphedema. • Subcutaneous abscess. • Septicemia. • Nephritis.
Treatment • Systemic antibiotics, especially penicillin, e.g. benzyl penicillin 600-1200 mg IV/6 hrs or cephalosporines. • Rest, analgesics.
Skin diseases related to coryneform bacteria Erythrasma
It is mild, chronic, localized superficial infection of skin by Coryn. Minutissimum. • Clinically: sharply-defined but irregular brown, scaly patches
usually localized to groins, axillae, toe clefts or may cover extensive areas of trunk & limbs. Obesity & DM may coexist. • Coral red fluorescence under wood’s light.
Treatment • Topical treatment with azole antifungal agents for 2 weeks or topical fucidin. • Erythromycin orally.