HORMON PANKREAS
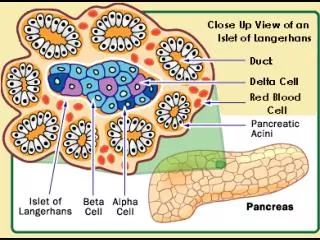
HORMON PANKREAS. SEL A ( ALFA) : HORMON GLUKAGON 25% SEL B (BETA) : HORMON INSULIN 70% DAN AMYLIN SEL D (DELTA) : SOMATOSTATIN < 5% SEL F ( γ ) : POLIPEPTIDA PANKREAS

HORMON PANKREAS
E N D
Presentation Transcript
HORMON PANKREAS SEL A ( ALFA) : HORMON GLUKAGON 25% SEL B (BETA) : HORMON INSULIN 70% DAN AMYLIN SEL D (DELTA) : SOMATOSTATIN < 5% SEL F ( γ ) : POLIPEPTIDA PANKREAS “ TRACE HORMONE “
AMYLIN Amylin or Islet Amyloid Polypeptide ( IAPP ) a 37 residu peptide hormone secreted by pancreatic beta cells at the same time as insulin Function : • Slow gastric emptying 2. Promote satiety 3. Inhibit secretion of glucagon during hyperglycemia
PADA GENETIK TERTENTU Amylin = IAPP = Islet Amyloid Polypeptide 1. Merusak sel beta pankreas 2. Menunjukkan efek antagonis terhadap hormon insulin pada tingkat reseptor yaitu menghambat pengikatan insulin pada reseptornya.
HORMON INSULIN ribosom endoplasmik retikulum PRE/ PREPROINSULIN PROINSULIN INSULIN DAN PEPTIDA C ( 95% ). golgi aparatus PROINSULIN : 1. MASIH PUNYA EFEK SEBAGAI HORMON INSULIN : 1-5%. 2. T1/2 > LAMA DIBANDING INSULIN 3. REAKTIVITAS BERSILANG TERHADAP INSULIN
Diabetes Mellitus is of 2 types Type 1 : is basically due to autoimmune mediated destruction of the pancreatic β islets resulting in insulin deficiency . Tx : exogenous insulin for survival and to prevent the development of ketoacidosis. Type 2 : is characterized by insulin resistance and usually associated with abnormal insulin production. People with NIIDM word wide will increase over 300 million 2025 .
What is the cause of IDDM? A. Degeneration of beta cells in islets from auto antibodies to beta cells, insulin, or enzymes in insulin synthesis B. Genetic deficiency in enzymes in the synthesis of insulin
What is the cause of NIDDM? Insulin resistance due to one of the following: • 1. decrease number of receptors in target tissue • 2. post receptor resistance/dysfunction • 3. increase IgG against insulin or receptor
1. Diabetes mellitus tipe I ( IDDM ) - Insulin darah menurun akibat kerusakan sel pakreas ok penyakit autoimmun - Usia dibawah 20 th, sering terjadi ketoasidosis 2. Diabetes mellitus tipe II ( NIIDM ) - Insulin normal / tinggi. Terjadi akibat resistensi insulin . Jumlah reseptor menurun. Jarang terjadi ketoasidosis - Usia diatas 40 tahun 3. Gestational diabetes mellitus - Diabetes mellitus yang terjadi pada waktu hamil
Diabetes Mellitus • Type 2 Diabetes • - blood glucose levels rise due to • 1) Lack of insulin production • 2) Insufficient insulin action (resistant cells) • - commonly detected after 40 • - effects > 90% • - eventually leads to β-cell failure • (resulting in insulin dependence) • Type 1 Diabetes • - cells that produce insulin are • destroyed • - results in insulin dependence • - commonly detected before 30 Gestational Diabetes 3-5% of pregnant women in the US develop gestational diabetes
Comparison of Type I and Type II Diabetes Mellitus Insert table 19.6
Obesity genes Derangement in inter -mediary metabolismEnvironmentOBESITY Insulin resis-tance gene Insulin Resistance β cell functionβ cell dysfunction and apoptosisβ cell dysfunction genes IGTEnvironment T2DM
PADA DM TIPE I • Aktifitas LPL menurun, TG tidak dapat dilepaskan dai kilomikron dan VLDL, sehingga terjadi peningkatan TG darah . • Mobilisasi asam lemak dari jaringan lemak menuju ke hati -----+ reesterifikasi ------+ meningkatkan sekresi VLDL ( fase awal ). Pada fase lanjut asam lemak akan membentuk benda keton -----+ ketoasidosis .
DIABETES MELLITUS SEKUNDER 1.AKROMEGALI 2. SINDROMA / PENYAKIT CUSHING 3. GLUKAGONOMA 4. FEOKROMOSITOMA 5. SOMATOSTATINOMA
Menifestasi Klinik Gejala awal umumnya yaitu ( akibat tingginya kadar glukosa darah) : o Polipagi o Polidipsi oPoliuri o Kelainan kulit, gatal-gatal, kulit kering o Rasa kesemutan, kram otot o Visus menurun o Penurunan berat badan o Kelemahan tubuh o Luka yang tidak sembuh-sembuh
KORTEKS ADRENAL 1. GLUKOKORTIKOID :DI SINTESIS DI ZONA FASI- KULATA ( PALING POTENT : KORTISOL ) . KORTIKOSTERON : DOMINAN PADA RODENT 2. MINERALOKORTIKOID :DISINTESIS DI ZONA GLOMERULOSA DAN ZONA FASIKULATA. 3. HORMON SEKS ( ANDROGEN ) : DISINTESIS DI ZONA RETIKULARIS DAN ZONA FASIKULATA .
KOLESTEROL 170H ASE P450 SCCP450C17 DESMOLASE PREGNENOLON 3 OHSD DAN 5-4 ISOMERASE PROGESTERON 21 OH ASE 11 DEOKSIKORTIKOSTERON 11 OH ASE KORTIKOSTERON 18 OH ASE 18 0H KORTIKOSTERON 18 OH DEHIDROGENASE ALDOSTERON
TRANSPORT HORMON ALDOSTERON DARAH TERIKAT LEMAH PADA ALBUMIN. MINERALOKORTIKOID LAINNYA TERIKAT PADA CBG.
ALDOSTERON DAN KORTIKOSTERON MAMPU MENGIKAT RESEPTOR GLUKOKORTIKOID SECARA SEMPURNA ( DIGOLONGKAN AGONIS ), NAMUN DALAM KEADAAN FISIOLOGIK TIDAK MENUNJUKKAN EFEK SEBAGAI HORMON GLUKOKORTIKOID. PADA KEADAAN KEKURANGAN ENZIM 17 HIDROKSILASE, MAKA HANYA KORTIKO- STERON YANG MAMPU MENUNJUKKAN EFEK SEBAGAI HORMON GLUKOKORTIKOID.
RESEPTOR MINERALOKORTIKOID TIPE I DAN II DIGUNAKAN MENGIKAT MINERALOKORTIKOID, TIPE II JUGA MENGIKAT HORMON GLUKOKORTIKOID. AFINITAS MINERALOKORTIKOID PADA TIPE IIISANGAT RENDAH. Ingat pada sindroma Cushing ataupun penyakit cushing terjadi efek mineralokortikoid dari hormon glukokortikoid yang meningkat
DIURETIKA SPIRONOLAKTON ( ALDAKTON ) DIGUNAKAN SEBAGAI DIURETIKA KARENA MEMBENTUK KOMPLEKS INAKTIF DENGAN RESEPTOR ALDOSTERON
AFINITAS ALDOSTERON TERHADAP RESEPTOR NYAKADAR ALDOSTERON DARAH LEBIH KECIL DPD KADAR DOC, KORTISOL DAN KORTIKOSTERON. NAMUN IKATAN ALDOSTERON TERHADAP RESEPTOR MINERALOKORTIKOID TIPE I LEBIH KUAT DPD IKATAN TERHADAP DOC, KORTISOL DAN KORTIKOSTERON OLEH KARENA:1. KADAR ALDOSTERON EFEKTIF LEBIH BESAR DPD KADAR DOC, KORTIKOSTERON ( BENTUK BEBAS ).2. RESEPTOR ALDOSTERON MENGANDUNG ENZIM 11 BETA OHSD YANG MAMPU MENGUBAH KORTIKOSTERON MEN- JADI SENYAWA YANG TIDAK AKTIF
ALDOSTERONISME I. ALDOSTERONISME PRIMER ( SINDROMA CONN) RENIN DAN ANGIOTENSIN II MENURUN II.ALDOSTERONISME SEKUNDER TJD PADA PENYAKIT SIROSIS HEPATIS, CONGESTIVE HEART FAILURE ATAU SINDROMA NEFROTIK. RENIN DAN ANGIOTENSIN II MENINGKAT GEJALA KEDUANYA : HIPERTENSI, HIPOKALEMIA, HIPERNATREMIA, ALKALOSIS
HORMON MINERALOKORTIKOID REGULASI MINERALOKORTIKOID A. SISTEM RENIN-ANGIOTENSIN ACE : 1. MENGUBAH ANGIOTENSIN I MENJADI ANGIOTENSIN II 2. MEMECAH BRADIKININ ANGIOTENSIN II :1. VASOKONSTRIKSI ARTERIOL ( cAMP ) 2. MERANGSANG PERUBAHAN ( VIA : Ca / FOSFATIDIL INOSITOL ) KOLEST --- PREGNENOLON b. KORTIKOSTERON------18 OH KORTIKOSTERON c. 18 OH KORTIKOSTERON----ALDOSTERON. B. KALIUM = ANGIOTENSIN II C. NATRIUM D. ACTH
The recent discovery of the G-protein-coupled receptor GPR91 which is activated by the citric acid cycle intermediatesuccinateprompted the discovery of a new, direct link between high glucose levels and renin release from the juxtaglomerular apparatus (JGA) in the kidney
Hyperglycemia is an important factor in cardiovascular damage, working through different mechanisms such asactivation ofprotein kinase C, polyol and hexosamine pathways, advanced glycation end products ( age ) REACTIVE OXYGEN SPECIES (ROS) ACCUMULATION ROS CAN DIRECTLY DAMAGE LIPIDS, PROTEINS OR DNA OXIDATIVE STRESS INDUCES ENDOTHELIAL DYSFUNCTIONTHAT PLAYS A CENTRALROLE IN THE PATHOGENESIS OF MICRO AND MACRO VASCULAR DISEASES NEFROPATI DIABETIK
DEFISIENSI INSULIN HIPERTROFI GINJAL PENINGKATAN TEKANAN INTRA KAPILER GLOMERULUS GLUMERULOSKLEROSIS TDS MENINGKATSTRESS MEKANIK STRESS FIBER PENGENDAPAN MATRIKS EKSTRASEL TGF β1( STIMULASI ANGIOTENSIN II ) VEGF , CTGF
HYPERGLIKEMIA1. POLIURIA , HIPONATREMIA, VOLUME DARAH2. GANGGUAN ENDOTEL ( MAKRO/MIKROVASKU-LER ) VASODILATASI RENAL HIPOTENSI3. SUKSINAT MENINGKAT +GPR91 PADA HIPERGLIKEMIASISTEM RENIN - ANGIOTENSIN - ALDOSTERON