Inhaler Devices
Inhaler Devices. Dr. Dane EDIGER Uludağ University School of Medicine Departement of Allergy. Inhalation Devices. Aim To make aerosol from the drugs solution or solid particles 1-Metered dose inhaler 2-Dry powder inhaler 3-Nebulizer. Definition of an aerosol. Aero air Sol solution

Inhaler Devices
E N D
Presentation Transcript
Inhaler Devices Dr. Dane EDIGER Uludağ University School of Medicine Departement of Allergy
Inhalation Devices Aim To make aerosol from the drugs solution or solid particles 1-Metered dose inhaler 2-Dry powder inhaler 3-Nebulizer
Definition of an aerosol • Aero air • Sol solution • Liquid or solid suspensions into gas medium • Particles which are sufficiently small so as to remain airborne for a considerable period of time
Lower aerosol size Upper aerosol size . 0,001 µm 0,01 µm 0,1 µm 1 µm 10 µm 100 µm =0,1 mm
History of Inhaled Therapy • China, India, Middle-east • Hippokrattes • Galenos • 4000 years ago: the smoke of ephedra sinica was used to asthma therpy • Smoke of Atropa belladona, Datura stramonium • Sulphur, arsenic, menthol, timol, eucaliptus
Modern age • Metered dose inhaler 1956 Medihaler • Dry powder inhaler 1960 • Multidose dry powder inhaler 1970 • 440 million boxes aerosols per year are manufactured in the world
Why Inhalation Therapy? • Targeted delivery of medication to the lungs • Rapid onset of action • Smaller doses • Less systemic and GI adverse effects • Relatively comfortable
PHARMACOKINETICS OF INHALED DRUGS Oropharynx absorbtion Lung absorbtion Gastrointestinal absorbtion SYSTEMIC CIRCULATION Vena porta Hepatic inactivation Urine elimination first pass effect
Deposition of particles > 5 µ impaction 1-5 µ sedimentation < 1 µ like gas
Hypothesis from available data Regional deposition Regional deposition Particle size (microns) Particle size (microns) Efficacy Efficacy Safety Safety Absorption from GI tract if swallowed Absorption from GI tract if swallowed Mouth / oesophageal region Mouth / oesophageal region > 5 > 5 No clinical effect No clinical effect Subsequent absorption from lung 1 – 5 Upper / central airways Clinical effect Some local clinical effect High systemic absorption < 1 Peripheral airways / alveoli
Lung deposition of drug • Particle • size • shape • particle density • solid or liquid phase • Type of inhalation device • Tecknique • Airway obstruction • Drug molecule
MDI/ DPI Small volumes Ready for use Stable obstructive disease Jet /Ultrasound nebulizer High fill volume > 1 ml Preparation required Severe respiratory insufficiency (asthma attack, COPD exac., CF) 4 Types of Inhaler Devices
Pressured Metered Dose Inhalers (pMDI) • Canister • Small reservoir • Metering reservoir • After pressure valve drug sprays • Aerosol
Metered Dose Inhalers (pMDI) • Canister • Propellent gas (liquid under pressure) • Drug • Dissolved or solid microparticules into the gas • Surfaktant • Physical stabilisation • Prevent clustering • Decreas valv friction • Drug layer is surface of liquid propellent because more lightweight, it must be rinced before use
Propellant Chloro fluoro carbon (CFC) • CFC (freon gas) • CFC not flammable • Vapouring after spray • Particules continue movement
Propellant Hydro fluoro alcan (HFA) • Not include chloride • Not disturbe Ozone layer • İt influence on global heating
MDI advantages • Rapid application • Handling • Multidose
MDI Disadvantages • Hand-breathe coordinations • İneffective use in poor ventilated patiens • Oropharyngeal deposition and local side effects • Not include dosimeter
MDI spacer Decrease of oropharyngeal deposition Proposing inhaled CS
Chest. 2002;121:871-876 The SmartMist was 100% accurate, The Doser CT was 94.3% and MDILog was90.1% All three devices are sufficiently accurate to monitor adherence in most clinical settings
Freon (CFC) • Cold freon effect • Oropharyngeal irritation, cough and bronchospasm • Harmfull for ozone layer • Cardiac arrhytmia • Less effective in cold climate
Evohaler Salbutamol Flutikazon BDP Levalbuterol Budesonide Formoterol MDI with HFA (CFC-free)
Therapeutic Ratio of Hydrofluoroalkane and Chlorofluorocarbon Formulations of Fluticasone Propionate Fowler SJ., Chest, 2002
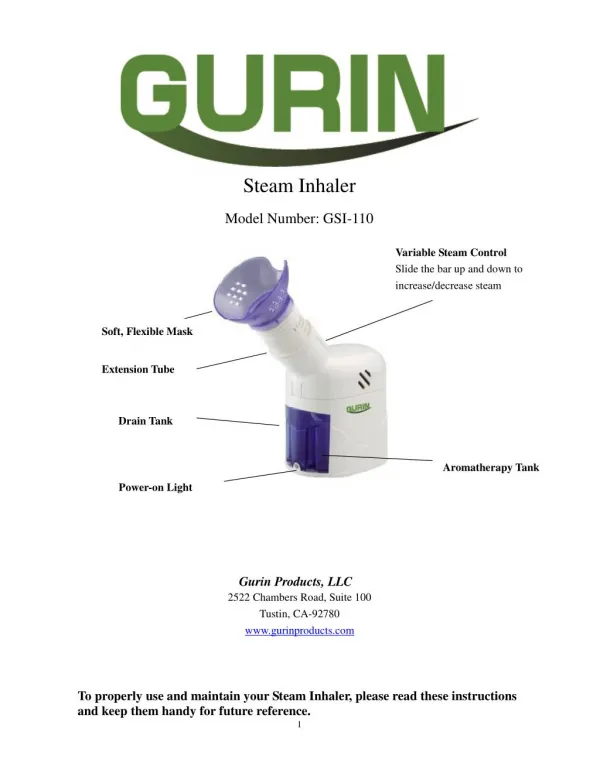
Classification of Dry Powder Inhalers, Based on Design and Function Single-Dose Devices Aerolizer formoterol capsule single HandiHaler tiotropium capsule single Multiple Unit-Dose Devices Diskhaler fluticasone blistercassette zanamivirblistercassette Multiple-Dose Devices Turbuhaler budesonidereservoir 200 Turbuhaler budesonide/formoterolreservoir 120 Diskus salmeterol blister strip 60 Diskus salmeterol/fluticasone blister strip 60
Lung depostion form a budesonide Turbohaler measured by gamma scintigraphy Borgstrom et al Eur Respir J 1994;7:69-73 Total lung deposition (% of inhaled dose) 30L/min 60L/min Inspiration Rate
FAST vs SLOW INHALATION USING 500mcg TERBUTALINE via A TURBOHALER (n=10 ASTHMATICS) FEV1, MMFR & PEFR FOR FAST > SLOW BUT N.S. LUNG DEPOSITION (% OF THE DOSE) 60L/min 30L/min Newman et al Int J Pharm 1991
Device dependent factors • Device • pMDI: • Portability, Treatment time, Drug preparation, Reproducibility, Coordination, Actuation, Drug availability, Holding chamber, Propellant • DPI: • Breath-actuation, Coordination, Portability, Treatment time, Dose counters, Flow requirement, Drug availability, Resistance, Costs. • Aerosol • Particle size, Velocity, Physico-chemical characteristics
Patient dependent factors • Age • co-operation • compliance • airway anatomy • breathing patterns • Disease
Lung Deposition of ICS Dose to the lungs MDIs Ciclesonide 52% Fluticasone 16% Budesonide 5-12% BDP HFA MDI 51% DPIs Different flow rates Budesonide Turbuhaler 17-39% Budesonide Novolizer 19-32% Budesonide Airmax 28-30% One flow rate Budesonide Clickhaler 27% Fluticasone Diskus 13%
TOTAL LUNG DEPOSITION AND DISTRIBUTION OF TERBUTALINE IN THE LUNG FOLLOWING INHALATION USING A TURBOHALER AND MDI CENTRAL ZONE INTERMEDIATE ZONE PERIPHERAL ZONE TOTAL LUNG % DEPOSITION MDI TURBOHALER Borgstrom & Newman Int J Pharm 1993;97:47-53
Mean intra-subject variability % coefficient of variability 60 52.0% 50 42.4% 40.4% 40 35.9% 31.8% 30 20 10 0 Volumatic Easi-Breathe Accuhaler Turbohaler Evohaler pMDI Device Aswania O et al. J Aerosol Med 2004; 17(3): 231-8.
a review looking systematically at the clinical effectiveness and cost-effectiveness of inhaler devices in asthma and COPD
Only randomized controlled trials (RCT) • (394 trials-years 1982 to 2001) assessing • inhaled corticosteroid, • B2-agonist • anticholinergic agents delivered by • MDI, • MDI with a spacer/holding chamber, • nebulizer, • DPI • Only 59 (primarilythose that tested B2-agonists) proved to have usable data
Results • None of the pooled meta-analyses showed a significant difference between devices in any efficacy outcome in any patient group for each of the clinical settings that was investigated • Theadverse effects that were reported were minimal and were related to the increased drug dose thatwas delivered • Each of the delivery devices provided similar outcomes in patients using thecorrect technique for inhalation
Aerosol Delivery of Short-Acting B2-Agonists in theHospital Emergency dept • SABA in the ED: nebulizer=MDIs with spacer • improving pulmonary function • reducing symptoms of acute asthma • inboth adult and paediatric patients (quality of evidence:good). • SABA in the ED: DPI = nebulizer=MDIs with spacer • in adults • data is inadequate(quality ofevidence: low) • Heart rate in the ED : nebulizer> MDIswith spacer (quality of evidence: good)
Recommendations • 1. Both the nebulizer and MDI with spacerare appropriate for the SABA in the ED • Qualityof evidence: good • net benefit: substantial • strength of recommendation: A • 2. Data for DPIs are limited • Quality of evidence: low • net benefit:none • strength of recommendation: I
The appropriate selection of a particular device in this setting • the patient’s ability to use the device correctly • the preferences of the patient for the device • the availability of the drug/device combination • the compatibility between the drug and the delivery device • the lack of time or skills to properly instruct the patient in the use of the device or to monitor the appropriate use • the cost of the therapy • the potential of reimbursement • Quality ofevidence: low • net benefit: substantial • Strengthof recommendation: B
Aerosol Delivery of SABA in theInpatient Hospital Setting • SABA in the inpatient:nebulizer=MDI with spacer • pulmonary function response (quality of evidence: good) • Recommendations: • 1. Both nebulizers and MDIs with spacerare appropriate for use in the inpatient setting • Quality of evidence: good • Netbenefit: substantial • strength of recommendation:A • 2. Data for DPIs are limited • Quality of evidence: low • net benefit:none • strength of recommendation: I
Aerosol Delivery of SABA for Asthma in theOutpatient Setting • SABA in the adult and paediatric outpatient:MDI=DPI • pulmonary functionresponses • symptom scores • heart rate • (quality of evidence: good) • SABAin the outpatient: MDI =MDI with spacer • pulmonary function responses(quality of evidence:low) • Data for nebulizers are limited • (quality of evidence: low)
Recommendations • 1. Both the MDI with or without spacerand DPIare appropriate for the SABA in outpatient • Qualityof evidence: good • net benefit: substantial • strength of recommendation: A • 2. Data for DPIs are limited • Quality of evidence: low • net benefit:none • strength of recommendation: I
Inhaled Corticosteroids for Asthma • Same dose of the same corticosteroid for adult patients with asthma in the outpatient: DPI or MDI with spacer • Pulmonaryfunction response • symptom scores (qualityof evidence: good) • Patient preference: DPI>MDI with spacer • 2 studies(quality of evidence:good). • Data for incidence oforal candidiasis ?? • (quality of evidence: low)