Download
1 / 22
260 likes | 1.98k Vues
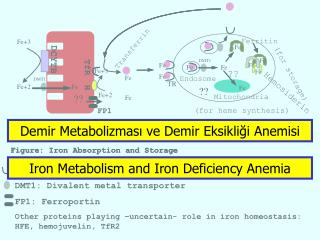
Demir Metabolizması ve Demir Eksikliği Anemisi. Iron Metabolism and Iron Deficiency Anemia. Deficiency of iron Anemia Hereditary deficiencies of enzymes of heme synthetic pathway Porphyrias. Figure. :. Iron Absorption and Storage. Ferritin. Fe+3. Fe. Transferrin. DCYTB. DMT1.

E N D
Demir Metabolizması ve Demir Eksikliği Anemisi Iron Metabolism and Iron Deficiency Anemia
Deficiency of iron Anemia Hereditary deficiencies of enzymes of heme synthetic pathway Porphyrias
Figure : Iron Absorption and Storage Ferritin Fe+3 Fe Transferrin DCYTB DMT1 Fe TfR Fe Fe Fe Fe Fe+3 Fe ?? (for storage) Fe Fe Endosome DMT1 TR H Fe+2 Fe ?? Fe Hemosiderin ?? Fe+2 Mitochondria Fe FP1 (for heme synthesis) Blood Normoblast Enterocyte TR: Transferrin receptor H: Hephaestin DMT1: Divalent metal transporter FP1: Ferroportin Other proteins playing –uncertain- role in iron homeostasis: HFE, hemojuvelin, TfR2
REGULATION of INTRACELLULAR IRON METABOLISM Sensors and Controllers of Intracellular Iron Supply= IRP-1 (Aconitase) & IRP-2 TF TR Fe Fe Fe Fe Fe Fe Crebs IRP-1 Fer Aconitase Stable TR mRNA Unstable TR mRNA Fe Fe Fe IRP-1 x Fe TR gene Fer gene TR gene Fer gene Healthy State Iron Deficiency
DEMİR HOMEOSTAZINDA ROL OYNAYAN BİR HORMON VAR MIDIR ? Hepatik Sinüzoid Endotel Fe Hepcidin Fe IL-6 Fe Fe Hepatosit Kupffer Fe x x
Hepcidin x Fe FP1 x Fe FP1
Causes of Iron Overload • Primary 1) Hereditary hemochromatosis (HFE- and non-HFE) 2) Hereditary atransferrinemia 3) Aceruloplasminemia • Secondary 1) Ineffective erythropoiesis (thalassemia, sideroblastic anemia) 2) Transfusional hemochromatosis (aplastic anemia, MDS, sickle cell anemia, end-stage renal disease) 3) Chronic dietary or medicinal intoxication 4) Alcoholic cirrhosis 5) Porphyria cutanea tarda Iron chelation therapy by DFO-infusion pump in a patient with thalassemia
HEPCIDIN in HEREDITARY HEMOCHROMATOSIS Surprisingly, serum hepcidin is decreased in HFE- and some kinds of non-HFE hereditary hemochromatosis. Probably, HFE plays a role in regulation of hepcidin production. Therefore, HFE disruption leads to decreased hepcidin production. Hepcidin HFE Ferroportin Iron sensing mechanism TfR2 Fe Fe Increased iron Fe Fe Fe
Iron Requirements in Males and Females of Various Ages (Iron Deficiency Anemia) Occurs If (Iron Intake < Iron Loss) mg
= microcytosis = hypochromia = anisocytosis PERIPHERAL SMEAR in IDA SERUM IRON PARAMETERS in IDA Iron: 5 mg/dL (60-150) TIBC (transferrin level): 467 mg/dL (250-435) Transferrin saturation: % 7 (15-45) Ferritin:2 ng/mL (15-200) Transferrin receptor level
Transferrin Saturasyonu, Total ve Serbest Demir Bağlama Kapasiteleri Nelerdir ? Serbest Demir Bağlama Kapasitesi = Serbest Transferrin Total Demir Bağlama Kapasitesi = Serum Transferrin Aktivitesi (~Düzeyi) Serum Demiri = Demir Bağlamış Olan Transferrin Transferrin Saturasyonu = Serum Demiri / Total Demir Bağlama Kapasitesi Transferrin Saturasyonu = Serum Demiri / (Serum Demiri + Serbest Demir Bağlama Kapasitesi)
Differential Diagnosis of IDA Other common causes of hypochromic microcytic anemia are; • Thalassemia trait • Anemia of chronic disease (anemia of inflammation) These two disorders may be confused with IDA. Generally history, CBC, serum iron parameters are enough to differentiate between them. Occasionally, Hb electrophoresis & bone marrow iron staining may be necessary.
Differential Diagnosis of Iron Deficiency Anemia Kronik Hst. Anemisi TS= % 14 Demir Yüklenmesi TS= % 100 İnefektif Eritropoez TS= % 85 Normal TS= % 15-45 Demir EA TS= % 5
Removal of the Underlying Disease (if present) Iron Supplementation (Iron pills, 200 mg/day on empty stomach in adults) Anemia generally resolves within 2 months, but iron pills should be continued until iron stores get full (~ 6-9 months) In the case of treatment failure one should consider: incorrect diagnosis, an additional cause of anemia, ongoing blood loss, bad patient compliance & malabsorption Indications for Parenteral Iron: Malabsorption Patient intolerance of pills Bad patient compliance to PO treatment Ongoing heavy blood loss Treatment & Follow-up in IDA
If the patient is at increased risk of IDA (e.g., women with suboptimal nutrition, infants, adolescents, pregnant women, women with multiple previous pregnancies) careful history, PE GUIAC test for occult GI blood loss & microscopic exam of stool for parasites will be sufficient. If suspicion of an underlying disease condition appears after simple tests or if the patient is a man or a postmenapausal woman the bowel, urinary and respiratory tracts must be carefully investigated for any bleeding lesion (e.g. peptic ulcer, colonic cancer). INVESTIGATION of THE CAUSE of IDA
Demir eksikliği anemisi bir halk sağlığı sorunudur. Dünya Sağlık Örgütü’nün verilerine göre dünya nüfusunun yaklaşık % 30 kadarı anemiktir ve bunların çok büyük çoğunluğu demir eksikliği anemisidir. Bu nedenle demir eksikliği anemisi için risk altındaki kişilere (gebelik, bazı infantlar) proflaksi uygulanması gereklidir: