Download
1 / 39
690 likes | 1.41k Vues
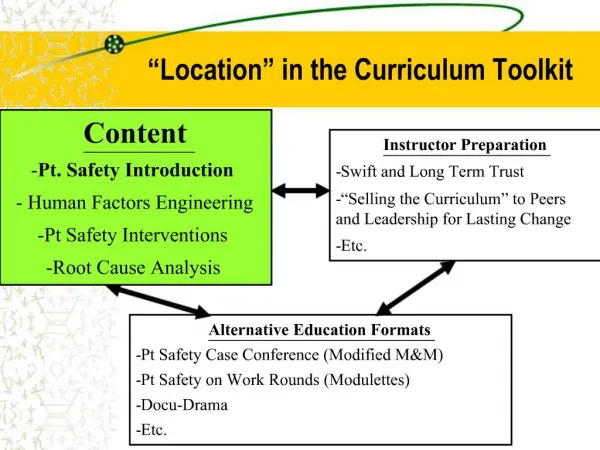
An Introduction to Principles of Patient Safety. Central Pennsylvania NANT Chapter Spring Conference – April 15, 2012 Gary Merica, R.Ph, MBA/HCM Director, Patient Safety, WellSpan Health. Objectives. Participants will be able to:

E N D
An Introduction to Principles of Patient Safety Central Pennsylvania NANT Chapter Spring Conference – April 15, 2012 Gary Merica, R.Ph, MBA/HCM Director, Patient Safety, WellSpan Health
Objectives • Participants will be able to: • Describe the frequency with which patients suffer unintended harm in hospitals • Define a culture of patient safety, and describe how to measure it • Describe 3 significant interventions hospitals can take to improve their culture of patient safety
Why?Numbers…………….. • 44,000 – 98,000 • 1 in 7 • 16 every quarter • 1.7 million • 99,000
……………and Names • Josie King • David Milne • Ben Kolb • Michael Colombini
Regulatory/legal “Stuff” • Pa Act 13 • Licensed practitioners required to report medical errors and adverse events to their organization • Organization must report events to the state • Written disclosure letters to patients/families for Serious Events
FOREIGN OBJECT RETAINED AFTER SURGERY AIR EMBOLISM BLOOD INCOMPATIBILITY PRESSURE ULCER STAGES III AND IV FALLS AND TRAUMA CAUTI CLABSI MANIFESTATIONS OF POOR GLYCEMIC CONTROL SSI DVT/PE AFTER HIP OR KNEE REPLACEMENT CMS Hospital Acquired Conditions
CMS Hospital Acquired Conditions • Since 10/1/08, hospitals do not receive the higher payment when: • One of these conditions is present as a secondary diagnosis at discharge • And was not present on admission • And results in a higher MS-DRG • In March 2011, 8 of the HACs were publicly reported on the CMS Hospital Compare website • Beginning in FFY 2015, hospitals in the worst performing quartile of HAC rates per 1000 eligible discharges will be subject to a 1% reduction in Medicare reimbursement.
Pa Act 1 of 2009: Preventable Serious Adverse Events Act • General rule: • A health care provider may not knowingly seek payment from a health payor or patient: • For a PSAE, or • For any services required to treat the problem created by the PSAE when the event occurred under their control
What is a “Culture of Patient Safety” • Culture • The predominating attitudes and behaviors that characterize the functioning of an organization…or • The collective behaviors, practices, and operational standards, driven by our shared values and beliefs…or • The way we do things around here • Safety • Freedom from unintended harm
Attributes of a Culture of Patient Safety • Patient centered, patient first • Mutual respect • Open communication • Highly functioning teams • Reporting and learning • “Just Culture” approach to safety • Peer accountability • Crucial Conversations • High reliability organization/practitioners
Patient CenteredMutual Respect • The American College of Physician Executives (ACPE) physician behavior survey: • 38.9 percent of the respondents agreed that "physicians in my organization who generate high amounts of revenue are treated more leniently when it comes to behavior problems than those who bring in less revenue.” 2. “There is a difference between hospitals that take care of patients and hospitals that take care of doctors.” 3. ISMP Intimidation Survey: • 40% of cliniciansfailed to intervene for patient safety due to fear of a negative encounter
Open Communication • 2010 AHRQ Survey on Patient Safety • Communication openness (62%) • staff will freely speak up if they see something that may negatively affect patient care (76%) • Or…..24 of 100 won’t • staff feel free to question the decisions/actions of those with more authority (47%) • Or….. 53 out of 100 don’t • staff are afraid to ask questions when something does not seem right (63%) • Or…..37 out of 100 are
Open Communication • Crucial Conversations • What makes a conversation “crucial”? • Stakes are high • Opinions vary • Emotions run strong
Highly Functioning Teams • Crew Resource Management • SBAR • Briefings/Time-outs/Debriefings • Critical language • Assertion • Situational Awareness • Checklists
Pre-procedure Briefing • Team introductions • Discuss patient, case – concerns • Team accountability • Set stage for open communication
Procedural Time-out • Immediately before incision or start of the procedure • Entire team is engaged, all activities cease (except life support) • Team positively affirms: • Correct patient • Correct procedure • Correct site • Note: 16 wrong site surgeries in Pennsylvania per quarter
Post-procedure De-briefing • Clinical/technical – counts, specimens, etc. • How did we do? • Any changes need to be made?
Peer Accountability • In the worst companies, poor performers are first ignored and then transferred • In good companies, bosses eventually deal with problems • In the best companies, everyone holds everyone else accountable – regardless of level or position
High Reliability Organizations • HROs have a preoccupation with the possibility of failure • Systems fail • People fail • HRO’s have a “healthy” recognition of these potential failures, and actively look to identify and mitigate them prior to patient harm
Why? • The single greatest impediment to error prevention is that “we punish people for making mistakes.” Lucian Leape, MD 1/25/00 Congressional Testimony
What Does the Data Show? • 2010 AHRQ Survey on Patient Safety: • Non-punitive environment (44%) • staff feel like mistakes held against them (51%) • Or…..49 out of 100 feel this way • feels like person being written up, not event (46%) • Or….54 out of 100 feel this way • staff worry that mistakes are kept in their file (35%) • Or…. 65 out of 100 worry about this
Who Supports This? • Organizations that advocate for adoption of a Just Culture: • National Quality Forum – 2009 Safe Practices for Better Healthcare: “A just culture should be fostered in which frontline personnel feel comfortable disclosing errors – including their own – while maintaining professional accountability.” • HAP – “HAP recommends that Pa hospitals and health systems strongly consider working with Outcome Engineering to implement a Just Culture model.” (12/05/08)
Who Supports This? • Organizations that advocate for adoption of a Just Culture: • Pa Patient Safety Authority • Institute for Safe Medication Practices • Joint Commission • Leadership Standard 03.01.01 • Leaders create and maintain a culture of safety and quality throughout the hospital • The focus of attention is on the performance of systems and processes instead of the individual, although reckless behavior and a blatant disregard for safety are not tolerated.
Just Culture • Unacceptable to punish all errors and unsafe acts • Equally unacceptable to give blanket immunity to all actions that contributed to an error – evolve from “blameless”, or “non-punitive” culture • Adjust the pendulum
Reporting and Learning • Principles: • Predicated on having a reporting environment in which staff feel comfortable and safe in reporting an observed risk or a mistake. • Looks to create a well established system of accountability • Recognizes that human beings are fallible, however also recognizes that in most circumstances we have control over our behavioral choices
Just Culture • Principles (cont.): • Based on “shared accountability” • Two inputs into good patient care: • Good system design (management responsibility) • Good behavioral choices (staff responsibility)
Measuring Patient Safety:Process, Structure, Outcome • Survey patient safety culture – process & structure • National Quality Forum – Safe Practices for Better Healthcare: “Healthcare organizations must measure their culture, provide feedback to the leadership and staff, and undertake interventions that will reduce patient safety risk”
Measuring Patient Safety:Process, Structure, Outcome • Observational methodology - process • Hand Hygiene – how good are we, and how do we know? • Crew Resource Management – are we just going through the motions? • ISO 9000 auditing requirements - It is considered healthier for internal auditors to audit outside their usual management line, so as to bring a degree of independence to their judgments.
Measuring Patient Safety:Process, Structure, Outcome • AHRQ Patient Safety Indicators (PSI), CMS Hospital Acquired Conditions – outcome • Preventable complications of hospital care • Iatrogenic pneumothorax • HAI • Blood incompatibility • PE/DVT
Change? Never doubt that a small group of thoughtful, committed citizens can change the world. Indeed, it is the only thing that ever has. Margaret Mead