Download
1 / 40
400 likes | 477 Vues
Explore how the Chronic Care Improvement Program (CCIP) is reshaping disease management strategies, evaluating efficacy, and influencing the future of healthcare delivery. Discover key issues, program design variations, evaluation methods, and stakeholder opinions.

E N D
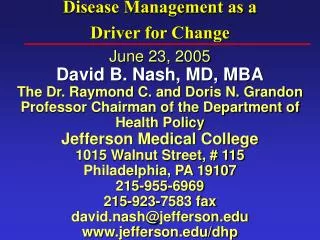
Disease Management as a Driver for Change June 23, 2005David B. Nash, MD, MBAThe Dr. Raymond C. and Doris N. Grandon Professor Chairman of the Department of Health PolicyJefferson Medical College1015 Walnut Street, # 115Philadelphia, PA 19107215-955-6969215-923-7583 faxdavid.nash@jefferson.eduwww.jefferson.edu/dhp
In 2004: Point with Pride View with Alarm End with Hope
Today’s Outline • CCIP (Medicare Health Support) Follow up: • Evaluation • DM Editorial Board • Generations at work • Future Issues
CCIP Evaluation • RTI International • Adequacy of the performance measures • Appropriateness of data sources
CCIP Evaluation Over-arching issues: • Claims databases • Patient self report • Chart reviews • Patient satisfaction scores • I.T. issues, legacy connectivity • Accreditation – JCAHO, NCQA, URAC
CCIP Program Design: Variation • Beneficiary outreach • Direct mail • Telephone • In-person visits • Risk stratification • Care Management plans • Services and educational materials
CCIP Evaluation CHF • To assess LVEF claims, chart review + self report • BP controlled • Use of ACE Inhibitors • Use of Beta Blockers PBM • Nutrition screening Data warehouse extraction
CCIP Evaluation Diabetes • Annual A1c test claims, self report and labs • Annual lipid profile • Annual eye exam • Monitoring for nephropathy
CCIPAssociated Organizations • Aetna – Active Health management • AMHWS • CIGNA – American Healthways • Health Dialog – Accenture
CCIPAssociated Organizations • Humana – Pfizer Health Solutions • Lifemasters –Express Scripts • Mckesson – Paradigm Health • VNSNY/UHCS – Evercare (part of United) • XLHealth – Omnicare Senior Services
CCIP Future • Timeliness • Measure of success • Politics • Public relations
DM Editorial Board Survey • What is your overall opinion of the Chronic Care Improvement Program (CCIP)? • How effective do you believe the program will be at achieving its goals? • What are the implications of the program for the DM industry? • If you were in charge of the CCIP, how would you judge its success?
What is your overall opinion of the CCIP? • The program is good in theory, but will be difficult to implement • The program is excellent and well designed • It is critical to the future of DM • It is great that the government is evaluating whether providing DM to the Medicare population makes sense and will provide value
Overall opinion, continued • The program is ground-breaking for DM and will force greater adoption of population-based models • This is an historical effort. It addresses a key issue – the current healthcare system underserves those with chronic conditions and is unprepared to meet future demands • The program will demonstrate the value of the DM strategies employed for the study populations
Overall opinion, continued • The intentions of the program are good: • Recognition of the more complex, long-term aspects of chronic care outcomes • Numerous options for enhancing chronic care • Utilization of coordinated processes to address chronic care • Utilization of population- and evidence-based approaches • Commitment to building on Phase 1 results for Phase 2 and the future
Overall opinion, continued • Some areas of concern • Program includes only limited populations and a few diseases • Will political pressure be exerted to demonstrate a pre-determined outcome? • Will CCIP be able to provide conclusive evidence of what works best and for whom? • Will true, uncontaminated randomization occur? • Will there be consensus on ROI methodology?
How effective will the program be at achieving its goals? • There is general acknowledgement that the programs are too important not to be succeed. The organizations involved will ensure that the programs are successful. • Program design will impact success. Population management programs are not prepared to care for the cohort of very ill people referred to them by CCIP.
Achievement of goals,continued • The program will improve certain outcomes for each disease, but demonstrated cost savings are unlikely. Satisfaction, high to begin with, will probably remain the same. • Failure is not an option. This philosophy will lead participant organizations to develop new and innovative strategies for managing patients with chronic diseases.
Achievement of goals,continued • Success will depend on program emphasis, implementation, and efficacy. There will be positive results for some measures, but no gain for others. • Some challenges • Good data • Ability to show outcomes • Stability of the populations • Large regions • Lack of provider network relationships
What are the implications of CCIP for the DM industry? • Implications will vary depending on the magnitude of the intervention. It will be difficult to prove value for the more complex, integrated interventions. • The implications could be significant. DM firms should focus on cost-effectiveness and efficient program implementation, as these are the key issues that will affect their opportunities as a result of CCIP.
Implications, continued • If the government expands DM programs, the implications are good. If the government cannot prove real savings via DM, it is likely that it will survive only as a quality tool. • The success of the CCIP is pivotal for DM. Health care in general follows the lead of CMS and Medicare. • If the CCIP program fails, it will have a chilling effect on the entire DM industry.
Implications, continued • CCIP will have a profound impact on the DM industry. CCIP encourages the DM industry to move positively toward innovative, scalable solutions. The effects of CCIP will be felt for years. • We can expect an increase in the number of new DM firms centered on the interventions indicated by CCIP, followed by the inevitable market consolidations.
Implications, continued • CCIP encourages DM firms to develop programs customized for its specific needs. These programs will not necessarily be applicable to other populations or delivery systems. The results of CCIP could be generalized in unintended and inappropriate ways.
If you were in charge of the CCIP, how would you judge its success? • CMS’s criteria should be expanded to include: • Detailed pre/post studies comparing costs and outcomes for the population before and after the intervention • Detailed cohort studies comparing like populations with the intervention against those without • Cost savings are paramount; programs must meet or exceed the goals.
Judging CCIP’s success,continued • Satisfaction is an important measure. A decline in satisfaction would have a significant impact because this population is generally fairly satisfied. • There should be focus on the special requirements of an elderly population (eg, support, stability, cognition, activities of daily living)
Judging CCIP’s success,continued • Cost-effectiveness is key. CCIP’s focus is on short-term outcomes. The challenge for CCIP will be to balance these data against indicators of potential long-term gains.
Employee Age Distribution Boomers 1946-64 Gen X Pre- Boomer Gen Y
47% over 50 would rather leave the health insurance decision up to the employer Want clear direction BABY BOOMERS Characteristics Benefit Recommendations Less choices o o Clear, concise communication o Education and communication o Higher income Targets on Replacement Ratio o o Loyalty to company Phased Retirement Benefits o o Depending on government (Social Security and Medicare) and company for retirement benefits Defined Benefit Retirement o o Healthcare o Education o o Not technology savvy Communication o Traditional Families Traditional Benefit Plans o o More prevalent bargaining groups Economies of scale o o Paying for children’s education Elder Care / Long Term Care o o Voluntary Life/Disability o 527 Plans o
Future of D.M. How Industries Change • Radical – Travel agencies; threat to the core • Progressive – Jet Blue, Southwest • Creative – Assets under threat, core activities stable; movies • Intermediating – Core assets stable, core activities threatened. Auction houses like Sothby’s Anita M. McGahan. HBR October 2004
Future of D.M. Intermediating Change Trajectory “Finding ways to preserve knowledge, band capital and other valuable assets while fundamentally changing relationships with customers and suppliers.”
Future of D.M. “Blue Ocean Strategy” W. Chan Kim and Renée Mauborgne HBR October 2004 Red Ocean – all industries in existence today Blue Ocean – all industries NOT in existence today Look back less than 30 years and think about overnight delivery, coffee bars, home video and mutual funds. Now, look ahead 10-20 years.
New ways of thinking Advances in biotechnology . . . Inst. Alt. Futures